Carpal Tunnel Syndrome – What is it?

Have you been experiencing pain, pins and needles or numbness in your wrist and hands, especially after using the keyboard, chopping up a few veges, reading a book, using your mobile phone or with driving?
If you answered yes – then you are most likely to have Carpal tunnel syndrome.
What is Carpal Tunnel Syndrome?
Carpal tunnel syndrome is the most common condition in the arm. It is caused by compression of one of the three major nerves in the forearm – the median nerve, which travels through the wrist into the hand and fingers. Entrapment of the median nerve usually due to inflammation, occurs in the wrist commonly resulting in tingling of the wrist and hand (in some cases forearm), numbness, pain and weakness of the hand.
Signs and Symptoms
Often unrelated to a specific incident or an injury, symptoms of carpal tunnel syndrome usually develop gradually overtime. Symptoms may be worse in the morning and night. Many people find that the frequency and duration of symptoms increase as the conditions worsen.
Signs and symptoms may include:
- Tingling, numbness or burning sensation of the thumb, index, middle and ¾ of ring fingers of the hand
- Electric shock like radiating pain through the hand into thumb, index, middle and ¾ of ring finger
- Weakened grip, loss of dexterity and fine movements such as picking up a hair pin, buttoning clothes.
- Hypersensitivity or in other cases lessened sensation of hand to pressure, heat or cold temperatures
- Swollen wrist
Let’s take a closer look at the anatomy!
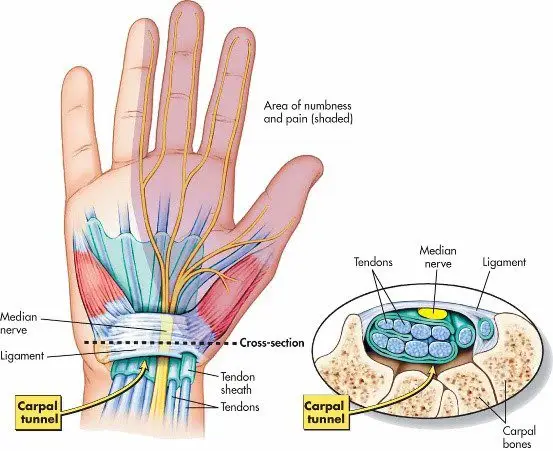
As its name suggests – a group of small bones aka carpal bones form a tunnel like passageway in the wrist (palmar view). This unique architectural design allows for the tendons of the forearm muscles and the all-important median nerve to pass through the narrow tunnel through the wrist and into the hand and fingers, supplying sensation and motor function.
Causes
Common causes and risk factors that increase the likelihood of carpal tunnel syndrome include:
- Repetitive wrist & hands movements – during work related tasks or leisure activities may irritate the tendons in the wrist, resulting in inflammation that irritates the nerve.
- Wrist or hand injury – recurring sprains, swelling and reduced wrist movements reduces the space in the carpal tunnel
- Pregnancy and menopause – hormonal changes can increase fluid retention in body increasing pressure in the carpal tunnel compressing the median nerve
- Genetic history – petite
- Medical conditions (rheumatoid arthritis, diabetes, hyperthyroidism)
Interesting facts about carpal tunnel syndrome
- Women are 3 times more susceptible to develop carpal tunnel syndrome than men. This can be due to hormonal changes during pregnancy or menopause and also because women tend to have smaller carpal tunnels.
- Not all fingers are affected. Median nerve supplies movement and sensation in the thumb, all fingers except the little finger.
- Computers/keyboard are not the only reasons to blame – repetitive nature of any work related or leisure word increases risk of developing carpal tunnel syndrome
Diagnosis
Carpal tunnel syndrome is fairly easily diagnosed by your physiotherapy, doctor or a hand therapist.
Your health practitioner will gather information on your general health, history and nature of your symptoms. They will then carefully conduct a thorough clinical assessment to assess the movements of your hand and wrist, strength and use a collection of tests in effort diagnose your symptoms. In some cases, your therapist may examine your neck, shoulders and arms to rule out other potential causes.
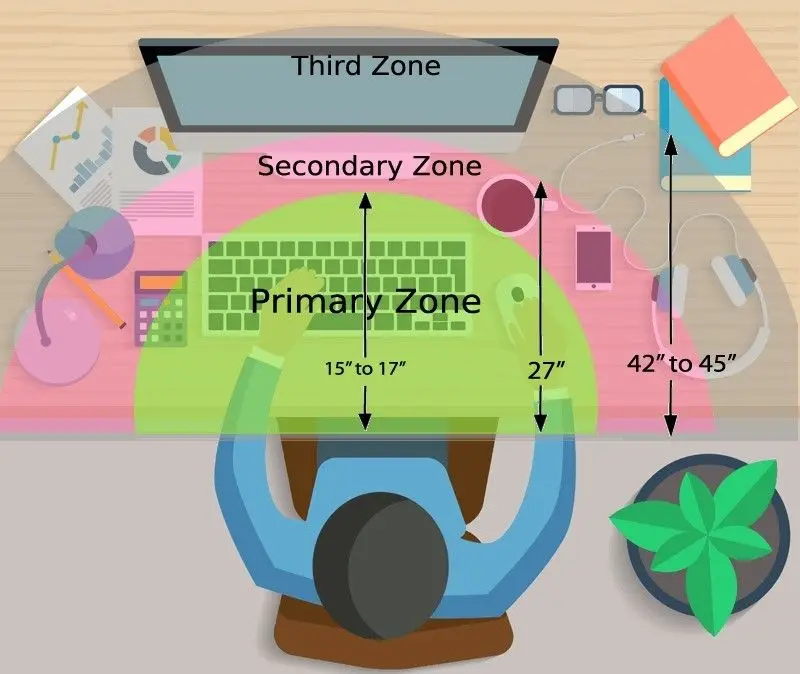
You may often hear the physiotherapist or hand therapist mention that they want to conduct a functional assessment – A functional assessment is activity specific, where the therapist will watch you perform the activity that aggravates your symptoms the fastest. For example, if using a keyboard is generally when you feel your symptoms start – the therapist may observe you performing the very task to examine your overall posture.
Referral to scans or nerve conduction tests may be arranged by your doctor or therapist depending on the severity or complexity of your symptoms.
Scans
Referral to scans or nerve conduction tests may be arranged by your doctor or therapist depending on the severity or complexity of your symptoms.
- Xray – provides key information on bone health, when dealing with a potential injury, or arthritis
- Ultrasound – can examine potential soft tissue injury or inflammation compressing the median nerve
- MRI – this advanced imaging provides in depth review of your wrist and hand. Usually arranged by your doctor or a specialist
- Nerve conduction study – studies the electrical activity of the median nerve. This test will help you doctor examine the severity of your problem.
Treatment
In most cases, carpal tunnel syndrome will progressively worsen overtime. So, the key is early intervention!
Conservative management
Mild symptoms can be easily managed with a conservative approach.
- Wearing splints or braces – keeps your wrist straight to prevent repetitive use of hands, thus reducing pressure or inflammation in the carpal tunnel.
- Non-steroidal anti-inflammatory medications – such as celecoxib and ibuprofen as prescribed by your doctor may decompress the median nerve by reducing the inflammation in your body and wrist.
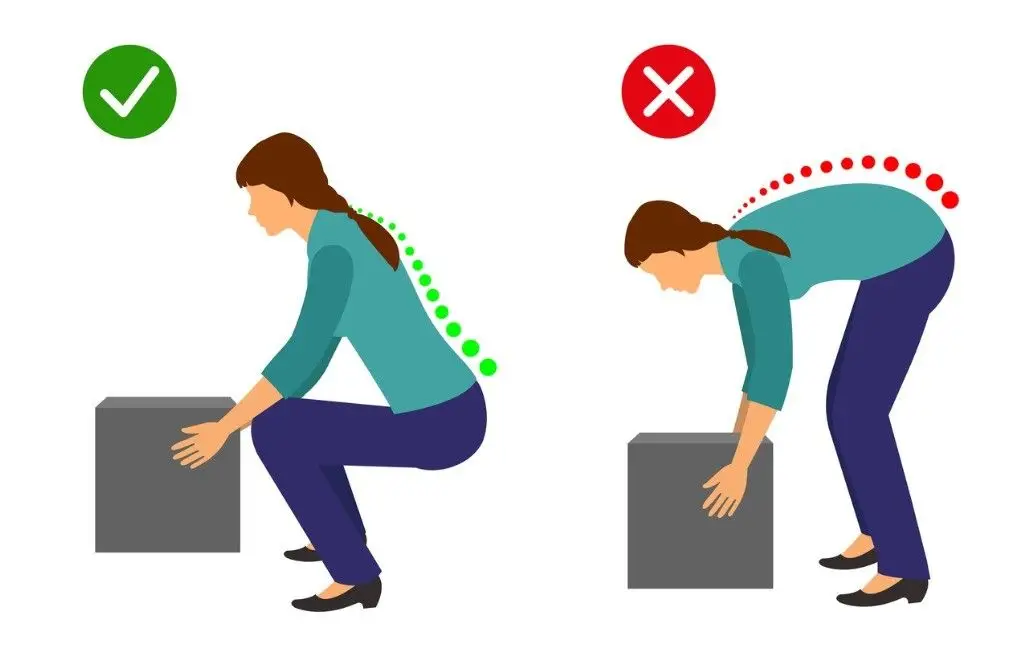
- Activity modification: your physiotherapist will play an important role in providing you with advice around to modifying your activities to reduce your symptoms. They will also prescribe you with effective stretches and exercises to help manage your symptoms while safely aiding your recovery.
- Steroid injections: your physiotherapist or doctor may recommend a ‘cortisone’, also known as a ‘corticosteroid’ injection to control your symptoms. It contains an anti-inflammatory substance that is injected into your carpal tunnel. The effects of the steroid injection may be temporary and can vary person to person depending on many factors (cause of symptoms, stage of your condition).
In mild to moderate cases, the effects of injection may last between 3-6months.
Surgical intervention
If non-surgical approaches have failed to relieve your symptoms, surgery may be required.
By this stage you would have consulted an orthopaedic surgeon. Your surgeon will thoroughly examine your overall health, symptoms, results from the scans and the nerve conduction study to help you decide on the best treatment approach.
If you decide to undergo surgery – the surgical procedure your surgeon will perform is called ‘carpal tunnel release’.
Recovery and outcomes
- After your surgery you may be given a splint or a brace for a period of time specified by your surgeon. While in the splint or brace you will be encouraged to move your fingers to prevent stiffness and swelling.
- Expect to experience minor pain, stiffness and swelling for a couple of weeks to months after your surgery. Pain medications provided by your surgeon must be taken as prescribed.
- You may be encouraged to see your physiotherapist, who will work closely with your surgeon to help meet post-operative outcomes.
- You will have regular 6-8 weekly follow ups with your surgeon as required to assess your healing and discuss gradual return to light activities and return to work.
- If you have underlying medical conditions such as arthritis, except that your recovery may be slower than otherwise expected. It is important that you follow post-operative protocols your surgeon, doctor and physiotherapist recommend.