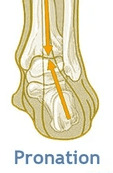
In the foot, pronation should occur naturally when the foot comes into contact with the ground. Pronation will appear as the foot rolling inward and the arch flattening.
What are the benefits?
Dissipates the force that the foot receives from the ground
Allows the foot to become a stable and mobile adaptor to enhance movement opportunity
Loads the muscles of the extensor chain (calf, quads, glutes) to convert ground reaction forces into forward momentum so we can propel efficiently.
So why have I been told this is bad?
So as you are now aware, pronation is very normal and a critical movement to ensure we move and propel ourselves forward efficiently.
What you may have heard someone say to you is that you ‘overpronate’?
Firstly, overpronation is subjective and not as black and white as it is sometimes made out to be. Overpronation has be defined as: ‘a foot that rolls inward toward the arch excessively’.
What we must understand is that a pronation can only happen when the foot has a stable tripod on the ground. This means that the calcaneus (heel bone), 1st metatarsal (big toe knuckle), 5th metatarsal (little toe knuckle) must all remain in contact when the foot rolls inwards and the arch flattens.
So, If you have been told you are ‘overpronated’ , it is most likely that your whole foot is ‘everting’ NOT ‘overpronating’.
What is Eversion?
Eversion can be defined as: ‘the process of turning inside-out’.
In pronation your heel must naturally ‘evert’ (sole of the heel will move away from the midline of the body) NOT your whole foot.
If your ‘whole foot’ everts (turns out) you will no longer have a stable foot tripod as the 5th metatarsal (little toe) will lose contact with the ground.
The key to ensuring this does not happen is to provide an environment for the bones of the midfoot (middle of the foot) and forefoot (toes) to experience the opposite motion to that of the heel. This will mean that the foot has an opportunity to truly pronate with a tripod on the ground.
So how can you help me do that?
At Physio fusion we can help you to bring your own body into alignment and create an environment in which the healing can begin
Foot strengthening exercises
Footwear advice
Referral to other healthcare specialists for further assistance (e.g. podiatrists)
To find your nearest Physio Fusion clinic and book an appointment call 09 6266186 or visit our websitehttps://physiofusion.co.nz
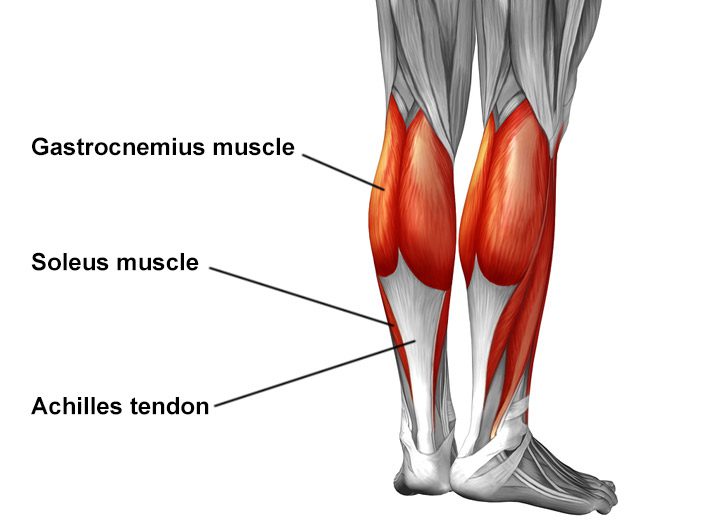
The Achilles tendon is the largest tendon in the human-body. It is a band of tissue that connects your calf muscles to your heel bone (calcaneus). This tendon primarily facilitates general mobility such as walking, running, climbing stairs, jumping, and standing on your tip toes, by helping to raise the heel off the ground.
Common Achilles Pathology
Achilles tendinitis and tendinosis are two common disorders and are typically classified as overuse injuries.
Achilles tendonitis involves inflammation of the Achilles tendon. Inflammation is the body’s natural response to injury or disease, and often causes swelling, pain, or irritation. This inflammation is typically short-lived. Over time, if this is left resolved, the condition may progress to degeneration of the tendon- Achilles tendinosis, in which case, the tendon loses its organized structure and is likely to develop microscopic tears.
There are two types of Achilles tendonitis and it is based on which part of the tendon is inflamed:
Insertional Achilles tendonitis affects the lower portion of your tendon where it attaches to your heel bone.
Non-insertional Achilles tendonitis involves fibres in the middle portion of the tendon and tends to affect younger people who are active.
In both non-insertional and insertional Achilles tendinitis, damaged tendon fibres may also calcify (harden) and often bone spurs (extra bone growth) develop with insertional Achilles tendinitis. Achilles tendonitis may also increase your risk of sustaining an Achilles tendon rupture (tear).
Causes
Typically referred to as “overuse” conditions, Achilles tendonitis and tendinosis are often caused by the sudden increase in repetitive activity involving the Achilles tendon. This can put too much stress on the tendon too quickly, that can then lead to micro-injury of the tendon fibres. Because of this ongoing stress on the Achilles, the body is not able to repair the injured tissue. The structure of this tendon is then modified, resulting in continued pain and other symptoms. The Achilles tendon also has poor blood supply that makes it more susceptible to injury and may make recovery from injury slow.
Common factors that may lead to the development of disorders of the Achilles tendon include:
Weak and/or tight calf muscles
Rapidly increasing the amount or intensity of exercise within a short span of time
Hill climbing or stair climbing exercises
Presence of bony spurs in the back of your heel
Changes in footwear – especially changing from wearing high-heeled shoes to flat shoes
Wearing poor fitting, inappropriate, or worn out shoes during sporting activities
Exercising without adequate warm-ups and stretching
A sudden sharp movement which causes the calf muscles to contract and the stress on the Achilles tendon to be increased. This can cause the tendon fibres to tear.
Excessive mobility
Poor feet positioning and biomechanics (excessive pronation and flattening of the arches of the foot)
Symptoms
Common symptoms include:
Pain and stiffness along the Achilles tendon especially first thing in the morning
Pain along the tendon or back of the heel that worsens with activity
Severe pain the day after exercising
Visible thickening of the tendon
Tenderness to touch
Bone spur
Swelling that is present all the time and gets worse throughout the day with activity
If you have experienced a sudden “pop” in the back of your calf or heel, you may have torn your Achilles tendon. Please seek urgent medical attention if you think you may have torn your tendon.
Diagnosis
If Achilles tendonitis or tendinosis is suspected, please deter from any activity or exercise which causes the pain. It is advisable to see your doctor or physiotherapist as soon as possible so that an accurate diagnosis may be made and appropriate treatment recommended.
You will be asked about the nature and duration of your symptoms and the medical professional assessing you will have a look at your foot and ankle. Ultrasound scanning may be used to evaluate the damage to the tendon and/or surrounding structures.
An MRI may be recommended if symptoms persist. X-rays may also be taken to rule out other disorders which may cause symptoms like Achilles tendonitis and tendinosis.
Treatment
Treatment will depend on the nature, severity, and length of the injury. Generally speaking, the longer the symptoms are present before treatment commences, the longer the timeframe until full recovery is attained. Full recovery may take between three and nine months.
Initial treatment options in the early stages may include:
Rest – to avoid further injury to the area
Ice – to reduce inflammation
Elevation – to reduce swelling
Non-steroidal anti-inflammatory drugs to reduce pain and inflammation.
How physiotherapy can help:
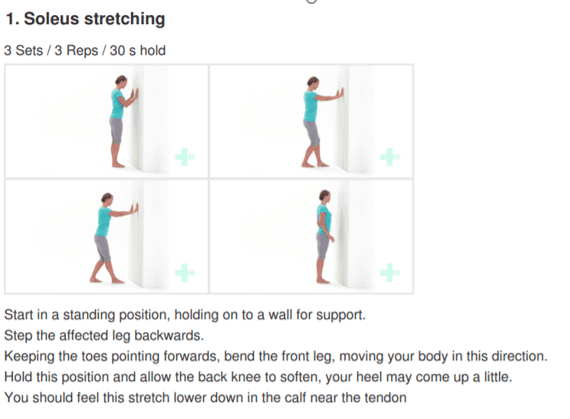
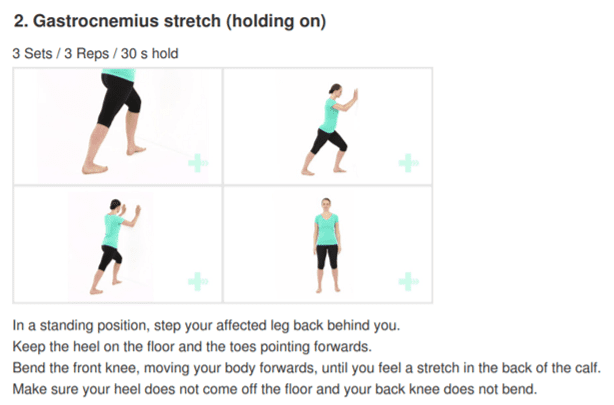
Physiotherapy typically focuses on two main areas: treatment and rehabilitation. Treatment may entail massage, shockwave therapy, acupuncture, gait re-education, and gentle stretching, whereas, rehabilitation predominantly entails strengthening of the Achilles and surrounding musculature.
Strengthening of the muscles surrounding the Achilles tendon facilitates healing in the tendon itself. Strengthening is attained through the utilization of specific exercises, that will be taught by your physiotherapist. It is common for the rehabilitation programme to take up to three months.