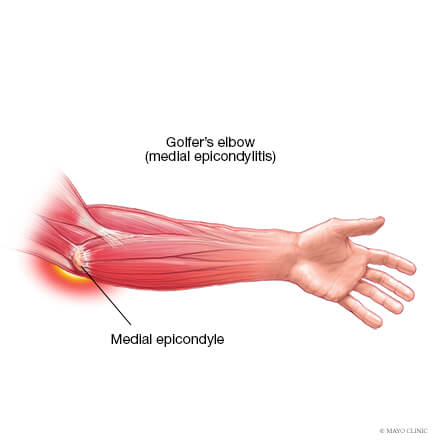
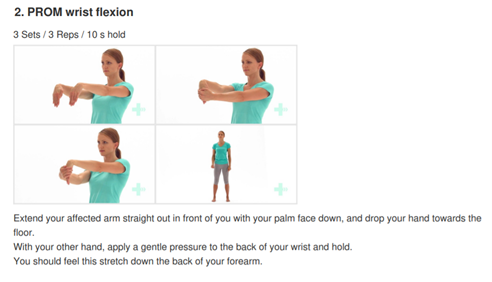
Medial elbow pain is also known as medial epicondylitis or golfer’s elbow. It is typically associated with pain on the inside (medial side) of your elbow and can spread into your forearm and wrist. This pain is the result of overloading and damage to the tendons that flex your wrist towards your palm.
Causes
This condition is triggered by damage to tendons and muscles which control your fingers and wrist. This damage is associated with excessive or repeated stresses- particularly repetitive and forceful finger and wrist movements, incorrect lifting, hitting and throwing techniques, lack of warmups and/or poor muscle conditioning.
Key risk factors for developing medial elbow pain may include smoking, obesity, being of in age bracket of 40 years old and over and undertaking repetitive activity with your arms for at least two hours daily. High risk occupations may include chefs, office desk workers, plumbers, construction workers, painters, butchers and assembly line workers. Those who partake in sports such as golf, racket sports, rowing, weight lifting and baseball are also at a higher risk.
Symptoms
Symptoms may be triggered suddenly due to a traumatic incident or may gradually develop over time and include but are not limited to:
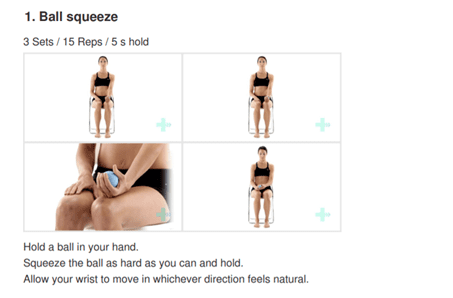
Tenderness and pain is typically felt on the inner side of your elbow (particularly on the bony knob), and may refer along the inner side of your forearm and down to your wrist and fingers. It often worsens with certain movements. For example, bending your wrist towards your palm against resistance, or when squeezing a rubber ball.
You may feel stiffness in your elbow, and making a fist may hurt
You may experience weakness in your forearm, wrist and hand
You may experience tingling and numbness that can radiate into one or more fingers — typically to your ring and little fingers.
Diagnosis
This condition is typically diagnosed based on your medical and occupation history and a physical exam by your doctor or physiotherapist. To evaluate stiffness, strength and pain, your clinician may apply pressure to the impacted region and get you to move your elbow, wrist and fingers in various ways. You may also be referred on for imaging such as X-rays and Ultrasounds to aid diagnosis.
Management
A mix of non-surgical treatment options are effective for the majority of medial elbow pain cases, and self-resolves over time. You should rest your elbow and painful activities should be avoided. But it is very vital to maintain gentle movements of the forearm, elbow, and wrist through its range of motion.
Potential treatment options include:
Ice
Rest
Physiotherapy and acupuncture
Anti-inflammatory medications as recommended by your doctor or pharmacist
The use of a wrist and forearm brace or splint to support and rest your forearm
As your initial elbow pain lessens, your muscles around the elbow, forearm and wrist should be safely strengthened and stretched under guidance of a physiotherapist. Your physiotherapist will advise you on particular exercises, give you appropriate symptom management advice and take you through a personalised graduated rehabilitation program. If you continue to experience pain after 6-8 weeks of treatment, your physiotherapist can refer you back to your doctors, to consider administration of a cortisone injection into the elbow to help reduce pain and inflammation, and further referral onto see a specialist to seek guidance on other treatment options.
Prevention
Having a good comprehension of risk of injury and being conscious of your everyday activities may aid in the prevention of medial elbow pain. You should:
Adopt appropriate technique and form when undertaking repetitive activities or sporting motions
Keep up with adequate wrist, forearm, and shoulder muscle strength
Undertake gentle wrist and forearm stretches pre and post activities
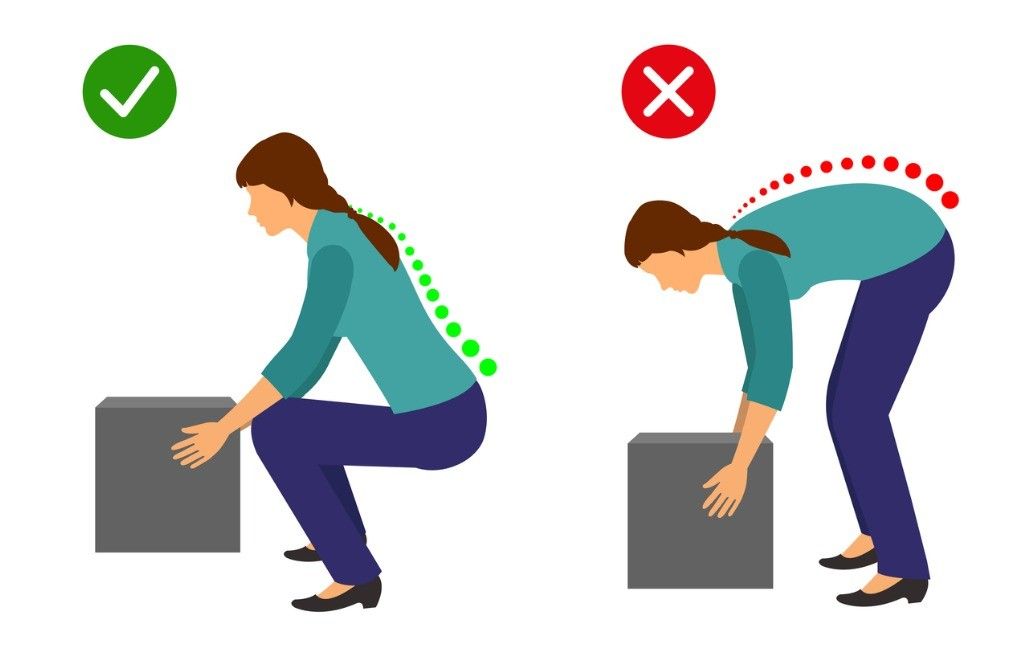
Adopt appropriate posture and body mechanics when lifting heavy objects to reduce joint strain- especially if doing so repetitively
RSI is typically defined as an overuse disorder- a gradual build-up of overload to nerves, tendons, and muscles arising from repetitive movements or activities. Repetitive use of the same motions leads to inflammation and damage to these soft tissues. This disorder mostly affects the upper limb- particularly the elbows, hands and wrists.
Causes
Possible causes of RSI include but are not limited to:
Undertaking the same and repetitive movements and stressing the same muscle groups
Working in cold environments
Assuming a sustained and/or awkward posture for prolonged periods of time
Undertaking a particular activity for prolonged periods of time with no rest-breaks
Frequent and prolonged use of vibrating equipment
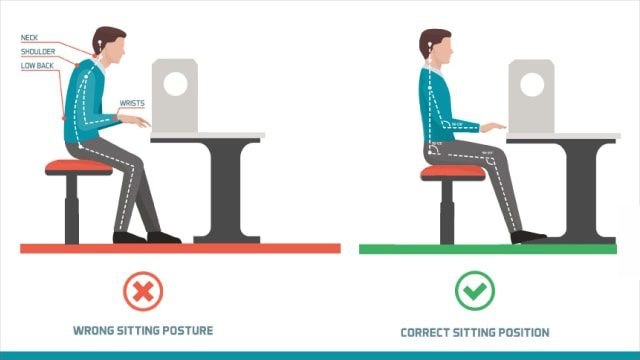
Adopting poor postures from working at inappropriately designed workstations
Undertaking a motion which involves carrying and/or lifting heavy items
Symptoms
RSI leads to a gradual development of a broad variety of symptoms, which range from mild to severe in severity. RSI particularly affects the muscles and joints of your wrists, hands, elbows, forearms, shoulders, neck. Having said this, RSI can affect other areas of the body as well.
Common symptoms may include:
Pain
Tingling
Cramping
Increased sensitivity to heat and cold
Tenderness
Fatigue
Loss of strength
Throbbing
Soreness
Achiness
Stiffness
Struggling with typical activities of daily living, such as gripping and twisting motions, carrying light weights, writing, kitchen prepping, dressing, personal cares etc
You may develop these symptoms when you undertake a task repetitively for a period of time, and can settle when you stop. Symptoms may settle over a few hours or over the course of a few days. However, if left untreated or is poorly managed, a minor RSI may gradually progress to a nasty chronic injury.
Diagnosis
If you experience mild discomfort whilst completing particular activities at home or at your job, it is a good idea to see your GP or physiotherapist to talk about RSI. But an RSI is not always simple to diagnose as there is no particular clinical test for it. Your GP will enquire about your medical history, occupation and work environment, and other activities to attempt to identify any repetitive motions you undertake that may be the cause of your symptoms. A physical examination will be undertaken, where they will assess your movement, check for pain, inflammation, sensation, tenderness, strength and reflexes in the impacted body part. RSI may be triggered by specific health disorders like bursitis, carpal tunnel, tigger finger, ganglion cyst, or tendonitis (inflammation in your tendons). Your GP can refer you on further diagnostic tests such as X-rays, Ultrasounds, blood tests, MRIs, nerve conduction tests etc, to determine if these underlying disorders may be the cause of your symptoms. You may be also be referred onto a physiotherapist and acupuncturist for conservative treatment and management for mild-moderate issues. If symptoms persist, you will then be referred onto a specialist.
Management
Initial treatment options for the management of RSI symptoms is conservative. This includes:
Rest, Ice, Compression, and Elevation (RICE principles)
Taking regular breaks between tasks and looking after your posture
Undertaking your activities and movements with appropriate form and posture
Intake of Nonsteroidal anti-inflammatory drugs (NSAIDs), both oral and topical as prescribed by the GP
Use of cold and heat to the impacted area
Administration of steroid injections into inflamed joints and tendons
Tailored exercise prescription from physiotherapists to correct posture and strengthen and stretch affected muscles
Acupuncture
Stress reduction and relaxation training
Use of splints and braces to help protect and rest the affected muscles and tendons
Ergonomically appropriate adjustments to your workstation and work environment may be recommended by your physio and GP- for example resetting your desk and chair if you’re working at computer, and alterations to your equipment and activities/motions to lessen the strain and stress on your muscles and joints. Surgery may be necessary in some cases.
Prevention
Minimizing repetitive actions particularly if they involve the use of heavy machinery or vibration. Improving your working posture and work-environment as well a taking regular breaks. Employers often undertake risk-assessments when you join a company to determine that the work area is ergonomically fit, comfortable and appropriate for you. You may be able to request for an assessment if you have not had one or are having issues with your work environment
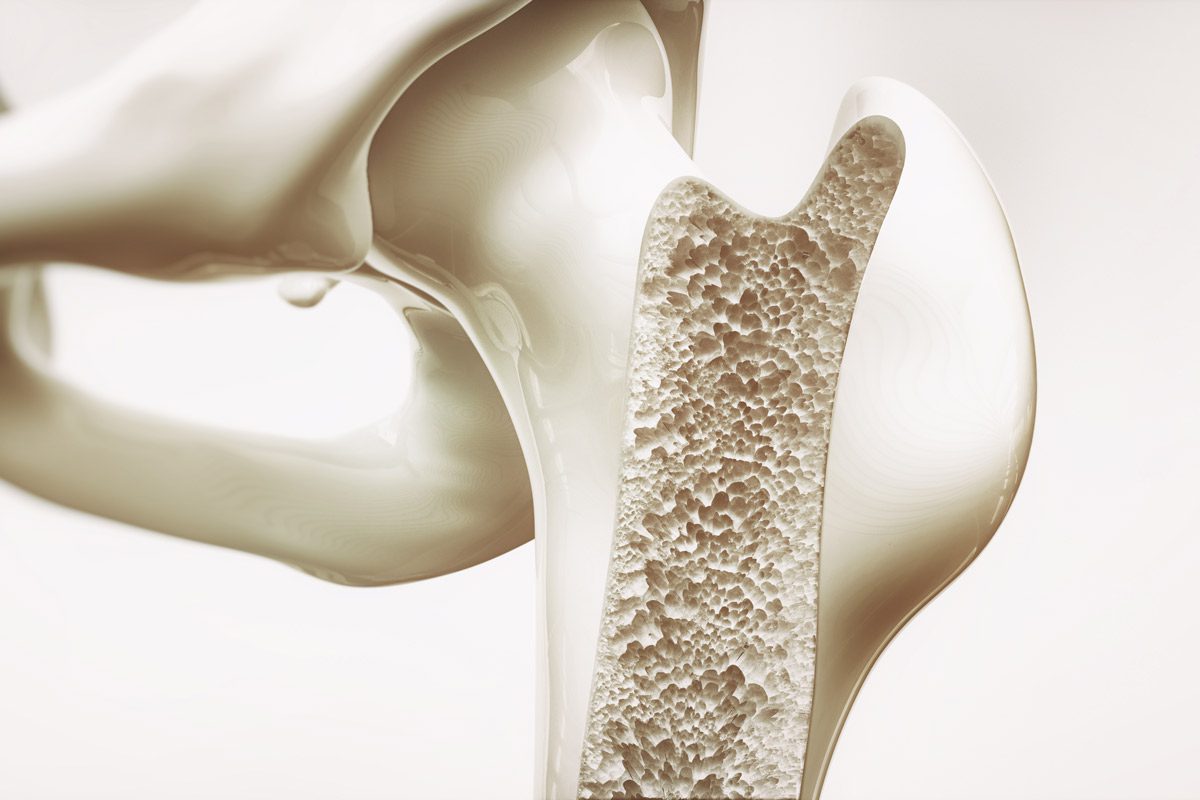
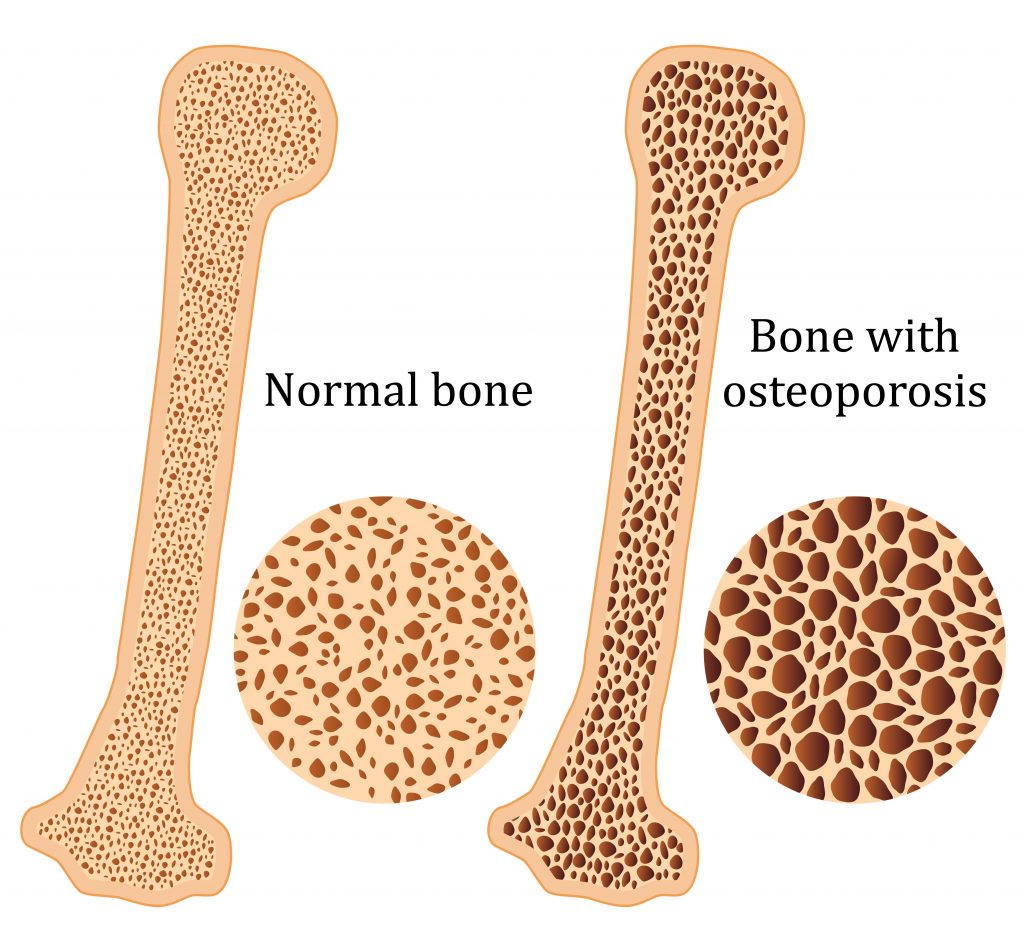
Osteoporosis is a condition which results in weak and brittle bones- to such degree that a fall or even mild stresses like coughing or bending over may result in a fracture. Bones are living tissues which are continually being broken down and replaced. However, your bones become osteoporotic when the formation of new bone does not keep up with the loss of old bone. This condition typically develops over time without any pain or other major symptoms, and is generally not diagnosed until you have sustained a fracture. The hip, pelvis, upper arm, spine and wrists are the most common structures affected by osteoporosis- related fractures.
How do you know if you have Osteoporosis?
Because there are no obvious early warning signs and symptoms, it is difficult to pre-diagnose osteoporosis. You may be unaware that you have this condition perhaps till you have one of the following:
Sustained a fracture from an incident more easily than you should have- like a simple fall or a bump
A decrease in the height of your spinal vertebrae over time
Change in posture – stooping or bending forwards
Back pain, due to a fractured or collapsed vertebra
Please see your doctor if you experience the following:
If you are over the age of 50 and have sustained a fracture
Sustained a spine, wrist, or hip for the first time
Sustained a fracture more easily than you should have (a simple fall or after a slight bump)
Risk factors
Key factors which may increase your risk of developing osteoporosis include:
Females- particularly post-menopausal Caucasian and Asian women
Over the age of 50
Excessive consumption of caffeine or alcohol
Smoking
Having a smaller or petite body frame
Poor physical activity levels and leading a very sedentary lifestyle
Family history of osteoporosis
Having low levels of vitamin D and poor dietary calcium intake
Decreasing levels of testosterone with ageing in men
Estrogen deficiency in women (irregular periods, early (before turning 40) or post-menopausal, surgical removal of the ovaries)
Use of long-term medication such as thyroid and epilepsy medications, corticosteroids
Having medical conditions such as gastrointestinal diseases; endocrine diseases; rheumatoid arthritis; cancer; and blood disorders
How will you be diagnosed?
Your doctor will review your signs and symptoms, family and medical history. You may be referred on for a specialized X-ray or CT scan to evaluate the bone density to help diagnose osteoporosis. Your bone density will be classified by comparing it to the typical bone density for a person of equivalent gender, size, and age.
How is Osteoporosis treated?
The treatment pathway chosen for the management of this condition is dependent on results of your bone density scan, gender, age, medical history and severity of the condition. Potential treatments for osteoporosis may include exercise, making positive lifestyle changes, vitamin and mineral supplements, and medications. Please consult your doctor for appropriate advice and treatment options.
How can Physiotherapy help?
Your physiotherapist will help you strengthen your bones and your muscles through a personalized and graduated rehabilitation program. Components of this rehabilitation program may include weightbearing aerobic exercises, resistance training using free weights/resistance bands/bodyweight resistance, and exercises to enhance posture, balance and body strength. Your physiotherapist will work with you to find activities that suit your needs and as per your physical activity level.
Although your knee has free movement going forwards and backwards, its’ sideward movements are restricted by the robust collateral ligaments on either sides of your knee. The medial collateral ligament (MCL) is situated on the inner part of your knee, but on the outside of your joint. The MCL connects the top of your shinbone (tibia) to the bottom of your femur (thighbone). It helps hold your bones together, provides stability and prevents your knee from bending sideways away from your body.
Injuries to the MCL are from the result of a direct blow to the outer part of your knee- and is most commonly seen in contact sports such as football and soccer. These injures may either over-stretch or cause a tear in the ligament. Whilst surgery may be needed in some severe cases, it is not always the go-to form of management.
Read on to know how physiotherapy can help manage your MCL related-knee pain.
Mechanism of Injury
Injury to the MCL typically occurs when a force drives the lower leg in a sideward direction away from your upper leg and body. Awkwardly landing from a height, twisting of your knee with your foot fixated to the ground, or from a direct blow to the outer part of your knee- most commonly seen in contact sports, are frequent causes of injury to the MCL.
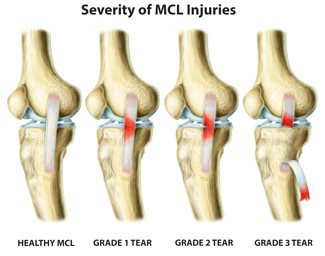
Grading of MCL Injuries
MCL injuries are often graded using the system below:
Grade 1: Regarded as a minor injury- means that the MCL has been overstretched but not torn
Grade 2: Regarded as a moderate injury- means that there is a partial tear in MCL, and presents with some degree of instability in the knee
Grade 3: Regarded as a severe injury- means that the MCL has completely ruptured/torn, and presents with noticeable joint instability
Often 3 MCL injuries are associated with concurrent medial meniscus and ACL ligament damage, which may need surgical intervention. But, the good news is that most MCL injuries may be treated well with conservative physiotherapy management. It usually takes between 2-8 weeks for Grade 1 and 2 MCL injuries to heal, and a graduated rehabilitation programme is highly commended for prevention of future injury.
Signs and Symptoms
Because injury to the MCL may present with similar symptoms as with other knee injuries such as ACL damage, it is vital to have a medical professional such as your physiotherapist evaluate your injury.
Common symptoms of an MCL injury may include:
Tenderness and pain along in the inner part of your knee
Swelling in the knee
Experience catching and locking sensations in the knee joint
A ‘pop’ sound at the time of injury
Actual or feeling of giving way of the knee (often indicate grade 2 or 3 injury)
Diagnosis
Your physiotherapist will discuss your injury and its presenting symptoms, past medical history (including a history of any prior knee injuries) and will also undertake a thorough physical examination. During the physical examination, your physiotherapist will assess the structures of your injured knee and compare them to the non-injured side. The range of motion, strength and stability of your knee will be assessed. You may be referred on for imaging such as X-rays and Ultrasounds to help aid the diagnosis. For more severe MCL injuries, and if your symptoms do not resolve with conservative physiotherapy management, you may be referred onto a specialist who may consider referring you for an MRI to get a deeper look at your knee.
Management
The management options for MCL injuries will be dependent on the severity of the injury. In the initial stages of injury, management is focused on controlling swelling and pain, whilst allowing your body to initiate healing processes via inflammation. This is typically achieved through the P.O.L.I.C.E. principles (Protect, Optimal Loading, Ice, Compression and Elevation).
Over the counter medication such as ibuprofen and paracetamol may be taken to reduce pain. Other stronger painkillers and NSAIDs may be prescribed by your doctor to help reduce swelling and inflammation as well.
After assessing your knee, your physiotherapist will frame a rehabilitation programme with exercises tailored to your needs. The purpose of physiotherapy is to help restore your knee’s range of motion, stability and strength, which in turn will then allow you to safely return to your usual day-to-day and sporting activities as soon as possible.
Management of most MCL injuries usually only involves knee bracing and physiotherapy treatment. However, in some cases, surgery may be recommended. Particularly if there is damage to more than one ligament or structure in your knee or if you continue to experience instability in spite of physiotherapy.
Rheumatoid arthritis (RA), a chronic inflammatory condition associated with swelling, pain, fatigue, and joint deformity. Although there are no known cures for this condition at present, a combination of treatments are available to help manage your symptoms. RA is the 2nd most common form of arthritis after osteoarthritis and is known to affect 1–2% of New Zealand’s population.
Signs and Symptoms
RA may develop very quickly or gradually over time, with its signs and symptoms, as well as the severity varying from one person to another. This condition is associated with episodes of remission and flare ups, with or without apparent triggers.
Other symptoms may include
Swollen, tender joints- (often accompanied by warmth and redness)
Joint pain
Joint stiffness which worsens in the mornings and after a period of inactivity
Fever, loss of appetite weakness, and fatigue
Muscle pain
Changes to the skin and nails
In the early stages of RA, you may notice its impact on your smaller joints- especially in your toes and fingers. And as this condition develops, your symptoms typically branch out to the bigger joints- your shoulders, ankles, knees, wrists, hips and elbows. Symptoms are likely to affect your joints bilaterally. Over time, RA also causes joints to deform and shift out of place.
Because RA is a systemic condition, it is estimated that approximately 40% of the RA population may experience symptoms and signs other body systems than the joints. These may include:
Kidneys, lungs, heart
Skin, eyes, mouth
Bone marrow
Nerves and blood vessels
Causes and Risk Factors
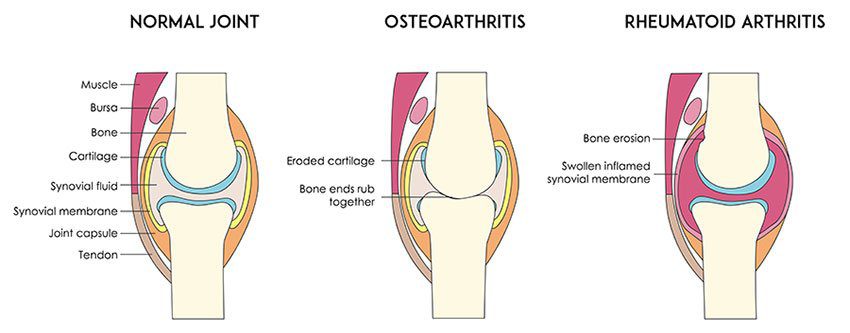
Your immune system is designed to help protect your body from infection and disease. However, in RA, changes occur in your immune system that (for poorly understood reasons), causes it to mistakenly attack the healthy soft-tissues of joints resulting in pain, swelling and inflammation. Because of this ongoing process, over time damages to the lining of your joints and other soft-tissues may lead to bone erosion and joint deformity. It can also have an impact on your heart, lungs, nerves, eyes and skin.
One can get RA at any age, although it is more probable to develop in those in the age bracket of 25-50 years old. Though rare, under 16s may also develop Juvenile RA or Still’s disease.
Risk factors for the development of RA include:
Family history of RA
Age bracket of 25-50 years old
Smoking
Women are more likely to develop RA than men
Obesity
Diagnosis
At present there is no single test to confirm a clinical RA diagnosis. It is often difficult to differentiate this condition in its initial stages from other forms of connective tissue inflammation (fibromyalgia, lupus, gout etc.).
Your doctor will get your full medical history (as well as any familial history of RA), discuss your signs and symptoms, undertake a physical assessment- particularly of your joints, and refer you on for imaging and blood tests. X-rays may help evaluate RA progression in your joints over time, whilst MRI and ultrasound imaging may help evaluate the severity of RA in your body. The blood test will evaluate your level of anti-bodies and proteins (including the rheumatoid factor protein that is present in approximately eighty percent of the RA population), and markers of inflammation.
Management
At present, though there is no cure for RA, a range of treatments are available which may help slow its’ progression and reduce pain and inflammation, minimise and/or prevent joint damage and maximise joint movement.
A combination of prescribed medication as advised by your doctor and other treatment options as noted below are recommended:
Cease smoking if you are smoker
Physiotherapy will help improve and maintain your joint range of motion, increase your muscle strength, and decrease your pain. Additionally, your physiotherapist or occupational therapist will be able to teach you ways of using your body efficiently to reduce stress on your joints
Finding a balance between rest and activity
Use of heat and cold packs to help ease pain and inflammation
The use of splints or braces for joint support as needed
Hydrotherapy- exercising in water reduces the pressure on your joints, whilst the warmth of the water will relax your muscles and help lessen your pain.
Seeking regular medical advice and check-ups to monitor your RA symptoms and the progression of the condition
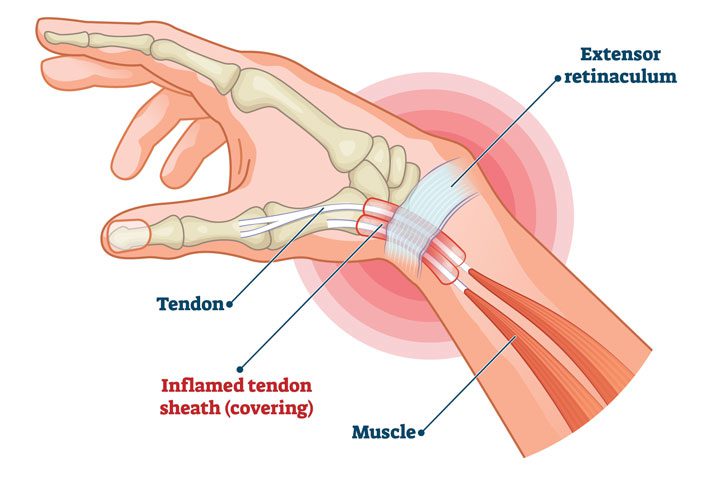
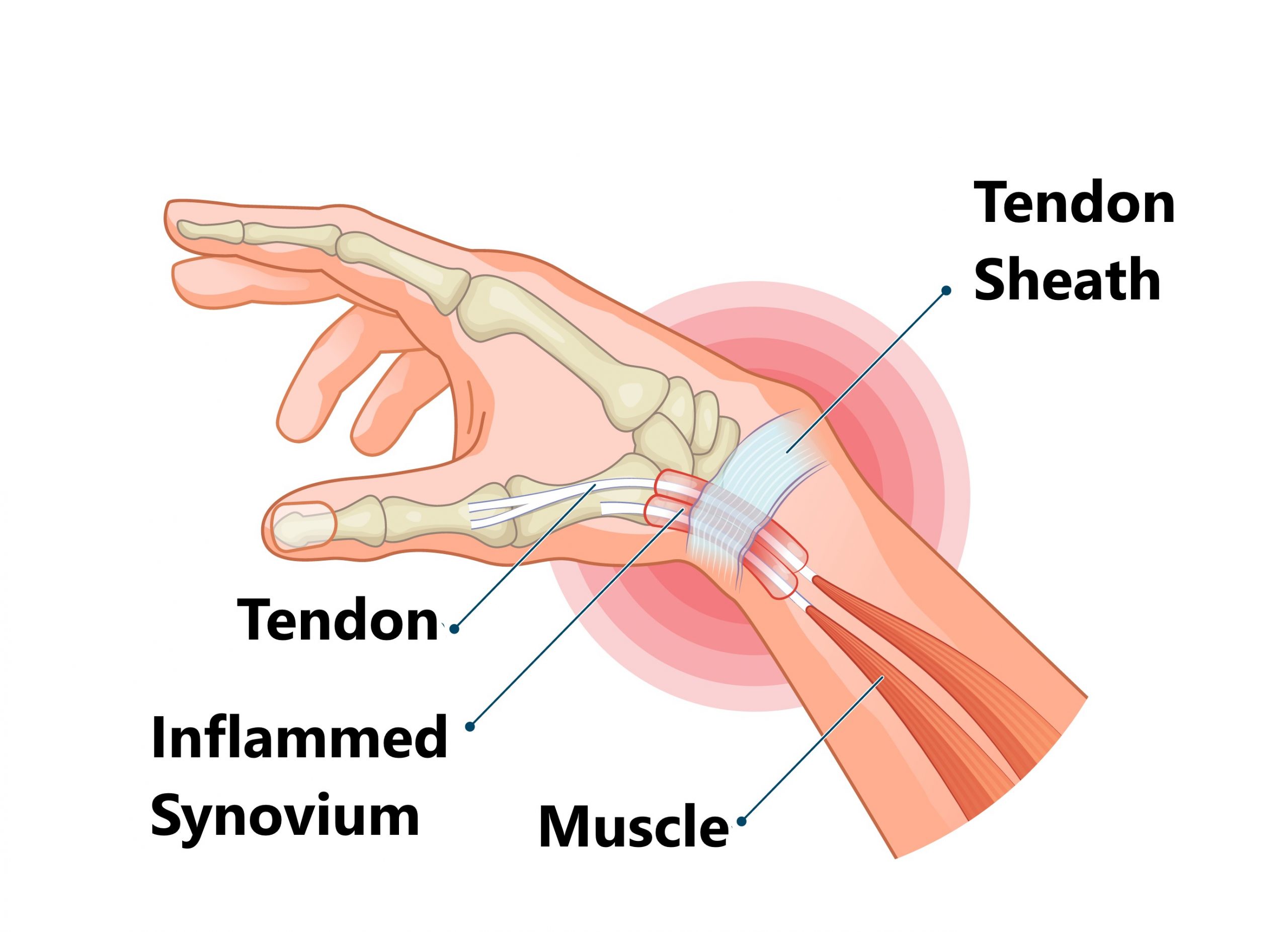
De Quervain’s tenosynovitis is categorised as an overuse disorder which affects the tendons in your wrist that you use to straighten your thumb. It is associated with swelling in the two tendons around the base of your thumb, which then causes the sheaths encompassing these tendons to become inflamed. This results in increased pressure on surrounding nerves as well, resulting in symptoms such as numbness, tenderness and pain. You are likely to have these symptoms when making a fist, gripping or grasping something, pinching, twisting your wrist, and/or laterally bending your thumb.
Symptoms
The key distinguishing symptom of De Quervain’s tenosynovitis is tenderness and/or pain at the base of your thumb. You can experience pain referring up or down your forearm. You may notice the pain gradually develop or appear suddenly, and worsen when using your wrist, thumb and hand. Painful movements include making a fist, gripping or grasping something, twisting your wrist, pinching, and/or laterally bending your thumb.
Other key symptoms include:
Swelling at the base of your thumb
Experience numbness along the back of your index finger and thumb
‘Snapping’ or ‘catching’ sensation experienced when you move your thumb
Causes
De Quervain’s tenosynovitis is typically associated with the chronic overuse of your thumb, hand and wrist. When undertaking movements like gripping, grasping, clenching, pinching, or wringing items in your hand, the two tendons in your lower thumb and wrist usually glide in a smooth manner via the small tunnel which attaches them to the base of your thumb. However, when you repeat a certain movement day in day out, it irritates the sheath around these two tendons, resulting in swelling and thickening which restrict their movements.
Factors which may increase your risk of developing this condition are:
Being in the age bracket of 30 to 50 years old
Pregnancy
Found more commonly in women.
Baby care: Lifting, carrying and/or holding your child repetitively with using your thumbs as leverage.
Hobbies or occupations which involve repetitive wrist and hand movements
Diagnosis
Your doctor or physiotherapist will discuss your medical and occupational history, and carry out a physical assessment of your wrist and hand.
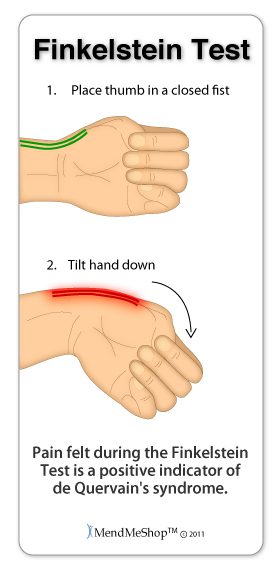
The physical examination will include palpation for pain when pressure is applied to the thumb side of the wrist, as well as clinical test called the Finkelstein test. This test requires you to bend your thumb across the palm of your hand and bend your fingers down over your thumb. You will then bend your wrist towards your little finger. If this causes pain on the thumb side of your wrist, you are likely to have this condition.
Whilst X-rays are usually not needed for the diagnosis, however, you may be referred on for ultrasound imaging.
Management
The aim of the management for this condition is to reduce pain caused by the irritation and inflammation of the tendons, preserve movement in the wrist and thumb, and prevent its reoccurrence. If treatment is commenced early, the symptoms should subside in 4-6 weeks. If your symptoms arise during pregnancy, they may settle around the end of the pregnancy or post the breast-feeding stage.
Splints may be utilised to immobilise and rest your wrist and thumb
Ice application to the affected area
Your doctor may recommend the use of anti-inflammatory medication to ease swelling and decrease pain
Avoiding pinching with your thumb when moving your wrist from side to side
Avoidance of aggravating repetitive movements and activities
Administration of corticosteroid injection into the tendon sheath can ease pain and decrease swelling if recommended by your GP
Physiotherapy: Your physiotherapist will examine how you use your wrist and provide suggestions on how to make technique modifications to relieve stress on your wrists. They will teach you strengthening exercises for your wrist, hand and arm to help decrease pain and limit tendon irritation
Surgery may be recommended by your specialist in more severe cases and if conservative management fails
Osteoarthritis impacts millions of people worldwide and is typically known as the most common form of arthritis. It is associated with the wear and tear of the protective cartilage which cushions the ends of your bones in your joints over time. Though this condition may cause damage to any joint in the body, osteoarthritis primarily impacts the joints in your spine, hands, hips, and knees.
Causes and Risk factors
Over time, the gradual deterioration of the cartilage which cushions the ends of your bones in your joints causes arthritis. Cartilage is a solid slippery tissue which allows almost frictionless joint movement. As the cartilage wears down, bone will eventually rub on bone.
This condition is typically characterized as a wear and tear degenerative disorder. However, in addition to the breakdown of the cartilage, it also impacts the joint as a whole. Osteoarthritis triggers alterations in the bone and damages connective tissue which holds the joint together and attaches your muscles to your bones. Inflammation of the lining of the joint is also triggered.
Factors which may put you at higher risk of developing osteoarthritis include but are not limited to:
Your age- the risk increases with getting older
Gender- though unclear why, but women are more perceptible to developing osteoarthritis
Bony deformities- those with abnormal joints or defective cartilage
Sustaining bony or joint injuries like those which take place during sport or from an accident.
The risk increases with obesity- the more you weigh, the greater your risk, as it adds more stress to your weight-bearing joints (particularly hips and knees)
Your occupation or a sport that you play which puts repetitive and excessive stress/loading on the joints, can eventually lead to the development of osteoarthritis.
Certain co-morbidities such as diabetes
Common symptoms
Below are some common examples of symptoms you may experience with arthritis. These may develop and worsen gradually over time
Pain: Your joints may hurt before and/or after undertaking an activity
Loss of joint range of motion– loss of overall joint flexibility and movement
Tenderness felt on applying light pressure to the joint
Joint stiffness that is most noticeable on waking up first thing in the morning or after a prolonged period of inactivity
Noticeable changes in joint pain with changes in the weather- particularly colder weathers
Sensations of grating and grinding// sounds of clicking and popping (crepitus) when you use the joint
You may notice swelling and redness around the joint, which may be triggered by soft tissue inflammation
Bony spurs that feel like hard bumps may develop around the impacted joint
How will I be diagnosed?
Osteoarthritis is typically diagnosed based on your medical and occupation history and a physical examination undertaken by your doctor. During the physical examination, your doctor will assess your affected joint(s) for swelling, tenderness, redness, and stiffness. X-rays may be recommended to reveal cartilage loss (the narrowing of the space between the bones of your joints), changes in bone, and bony spurs around the joint. Blood tests may be used to rule out other causes of joint pains like rheumatoid arthritis. Joint fluid analyses may also be used to test for inflammation to ascertain if the pain is triggered by an infection or gout instead of osteoarthritis.
Management
Though there isn’t a cure for osteoarthritis, various treatments which can help relieve symptoms of pain and disability are available.
Lifestyle modifications: Changes to your daily life may protect your joints and slow the progression of osteoarthritis. Minimising activities which exacerbate your symptoms such as climbing stairs, squatting. Swapping high-impact activities like running and jogging to lower-impact activities such as cycling or hydrotherapy will decrease the stress on your joints. Weight-loss reduces the stress and loading on your joints, which then results in less pain with increased function.
Assistive aids: Using assistive aids like a stick/cane, wearing proper shoes w orthotics and supportive braces/sleeves may improve your stability and support your functional capabilities.
Physiotherapy: Targeted exercises may help improve your flexibility as well as build strength in your muscles. Your physiotherapist will develop a personalised active rehabilitation program which is safe and will meet your requirements and lifestyles.
Medications: Various kinds of medication (such as paracetamol and NSAIDs) maybe helpful in treating and controlling the symptoms of osteoarthritis. As everyone responds differently to medications, your doctor will prescribe medicines (type and dosage), which is safe and will work best for you.
Cortisones: Strong anti-inflammatory agents which is injected into the affected joint to give pain relieve and decrease inflammation for a short period of time. Due to potential side-effects, it may be recommended to restrict the number of injections to 2-3 per year.
Other: Heat and ice applications, self-massaging with pain-relieving creams/ointments and/or wearing elastic supports may provide some relief from your pain and give you support.
Surgery: Surgery may be recommended if there is considerable degeneration in your joints and/or if your osteoarthritic pain causes disability that is not relieved with conservative management. Your doctor or specialist will discuss your options with you.
Tennis elbow, or also known as lateral epicondylitis, is a painful disorder of the elbow triggered by overuse. This disorder is characterised by inflammation or, in some cases, micro-tearing of the extensor tendons which link the forearm muscles on the outer part of the elbow. This leads to pain and tenderness on the outside of the elbow, spreading through to the forearm and wrist.
Causes
Tennis elbow is characterized as an overuse and muscle strain injury. It is caused by repetitive and/or vigorous contractions of the forearm muscles which is used to straighten, extend, and lift the wrist and hand. The repetitive motions and stress to the tissues can result in a string of tiny, microscopic tears in the tendons which attach your forearm muscles to the bony prominence on the outside of the elbow.
Tennis elbow may result from number of activities including but not limited to:
Typing and repetitive computer mouse use
Cutting/chopping motions
Manual work that involves repetitive turning or lifting of the wrist, such as plumbing, or bricklaying.
Gardening
Using hand tools such as scissors, clippers, screwdrivers, plumbing and carpentry tools
Playing racquet sports, such as tennis, badminton, or squash
Throwing sports, such as the javelin or discus
Painting
Sewing/knitting
Tennis elbow may also occur after a sudden knock or bang to the elbow, if you undertake activities that you are not used to excessively and aggressively, and sometimes there is no apparent cause for it.
Risk Factors
Factors which may increase your risk of tennis elbow include:
Your age: Whilst this disorder impacts people of all ages, it is mostly prevalent in adults in the age group of 30-50 years old.
Your occupation: Those who have jobs which entail repetitive movements of the wrist and arm are more likely to develop this disorder. Examples include but are not limited to painters, computer users, plumbers, butchers, carpenters, and chefs.
Sports: Partaking in racket sports increases the risk of tennis elbow, particularly if you use poor form and technique.
Common Signs and Symptoms
Pain noted around the bony knob on the outside of your elbow is the most common characterising symptom of tennis elbow. This knob is where the injured tendons connect to the bone. The pain is often depicted as “burning” in nature. Your elbow may be tender and sore to touch, and the pain can refer down to the forearm. The pain often increases with gripping, grasping, or rotating motions of the wrist and forearm. Bending and straightening your elbow may also be painful.
The severity of your pain may vary from a mild discomfort to severe pain that can interfere with your sleep and day to day activities. The pain typically starts gradually and then worsens over weeks or months.
Diagnosis
During your physical examination your physiotherapist will attempt to produce your pain in your elbow via specific tests and movements. They will assess your range of motion in your elbow, wrist, and shoulder joints. Referrals for X-rays and ultrasound scanning may be indicated to further support your diagnosis and to rule out other potential sources of your pain
Management
A mix of non-surgical treatment options are effective for the majority of tennis elbow cases, and self-resolves over time. You should rest your elbow and painful activities should be avoided. But it is very vital to maintain gentle movements of the forearm, elbow, and wrist through its range of motion.
Potential treatment options include:
Ice
Rest
Physiotherapy and acupuncture
Anti-inflammatory medications as recommended by your doctor or pharmacist
The use of a wrist and forearm brace or splint to support and rest your forearm
As your initial elbow pain lessens, your muscles around the elbow, forearm and wrist should be safely strengthened and stretched under guidance of a physiotherapist. Your physiotherapist will advise you on particular exercises, give you appropriate symptom management advice and take you through a personalised graduated rehabilitation program. If you continue to experience pain after 6-8 weeks of treatment, your physiotherapist can refer you back to your doctors, to consider administration of a cortisone injection into the elbow to help reduce pain and inflammation, and further referral onto see a specialist to seek guidance on other treatment options.
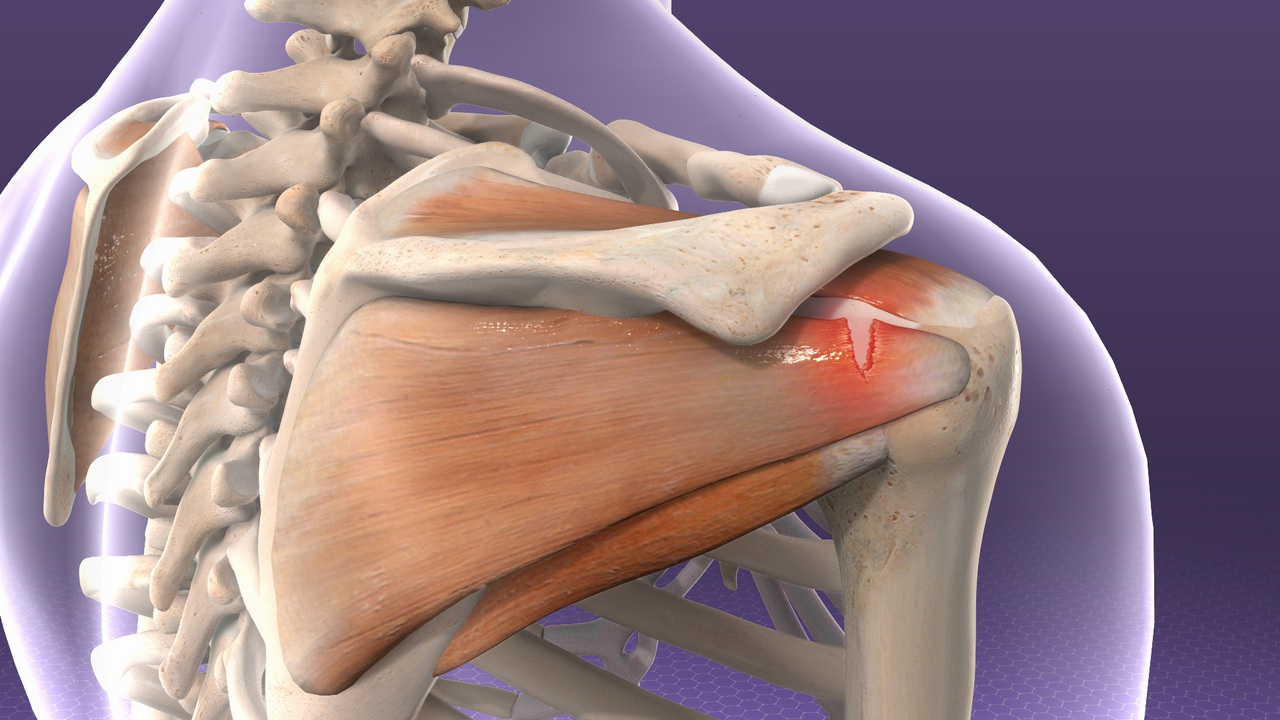
Rotator cuff injuries are the most common source of shoulder problems. They can range from minor sprains causing impingement type symptoms, to massive tears resulting in severe loss of function and pain. They commonly occur as a result of acute injuries (sports, falls), chronic overuse (repetitive loading) or due to gradual aging.
Anatomy of shoulder
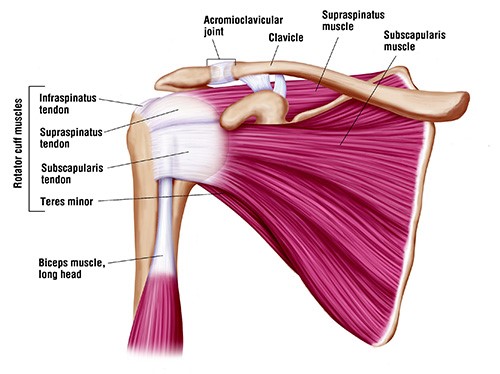
The shoulder joint (glenohumeral joint) is the most mobile joint in the human body. It comprises of the humeral head (top portion of upper arm bone) which fits in the glenoid cavity of the scapula (shoulder blade) to create a ball and socket configuration. This anatomical configuration results in limited bony contact between the humeral head and the glenoid fossa, which reduces the stability of the joint.
Several passive and active structures stabilize and maintain proper biomechanics of the shoulder joint.
Passive stabilizers include the ligaments, joint capsule, cartilage and the bony concavity of glenoid fossa. Thick cartilage known as labrum lines the glenoid fossa to further deepen the groove by about 50% which is advantageous in stabilizing the shoulder joint during the articulation.
Dynamic stabilizers of the glenohumeral joint is gained from the coordination of rotator cuff muscles that compress the passive structures providing stability and mobility as whole.
The rotator cuff muscles include:
supraspinatus
infraspinatus
subscapularis
teres minor
Injury to any or all these four muscles, including the tendons that attach the muscles to bone can result movement dysfunction and severe pain.
Other important joints of the shoulder complex include:
sternoclavicular joint
arcomioclavicular joint
scapulothoracic joints
Types of rotator cuff pathology
Tendinitis and Tendinosis
More often than not the term tendinitis and tendinosis are interchangeably used to describe a similar tendon pathology. However, the factor that differentiates the two is the time of injury (acute or chronic).
Tendinitis results from acute injury to the tendon which sets off an inflammatory process characterized by pain, swelling, and redness. On the other hand, tendinosis is a chronic pathology that does not involve an inflammatory process. It is characterized by degeneration of collagen fibers in response to persistent micro-trauma, vascular compromise and aging.
Acute rotator cuff tear
Acute tears result from sudden forceful lifting of the arm against resistance or in an attempt to cushion a fall (for example, heavy lifting or a fall on the shoulder).
Chronic injuries
Most commonly resulting from occupational or sports requiring excessive repetitive overhead activity.
Signs and symptoms
Symptoms of a rotator cuff injury are due to the inflammation that accompanies the strain. Swelling that forms within the small space of the joint prevents the normal mechanics of the shoulder, resulting in the clinical picture of pain and decreased range of motion.
Acute rotator cuff tears
Tearing sensation
Immediate severe localised pain
Reduced strength
Symptomatic clicking
Reduced and worsening pain with movements
Affects daily activities (personal care, lifting, reaching etc)
Chronic rotator cuff tears
Generalized deep dull ache, sharp onset of pain with movements
Global shoulder weakness
Reduced movements and daily activities (especially moving to the side, reaching behind back)
When to seek medical treatment
See your doctor or a physiotherapist if you experience any of the following symptoms in the shoulder:
Pain, especially pain that does not improve with rest
Swelling, redness or tenderness around the joint
Shoulder weakness
Reduced shoulder movement
For more severe rotator cuff injuries, you may require immediate medical attention.
Seek immediate medical attention if you experience the following symptoms:
Sudden, severe pain
Visible joint deformity
Inability to move or use your shoulder joint
Sudden swelling, discoloration
Diagnosis
To diagnoses an injured rotator cuff, your physiotherapist will begin with a thorough subjective and physical examination of your shoulder.
Subjective assessment
Your physiotherapist will begin with a thorough subjective assessment inquiring about your signs and symptoms of an acute injury as well as any symptoms that may suggest a more long-term problem.
Physical assessment
The physical examination often involves observation to look for muscle wasting, deformities, and/or changes in appearance of the injured shoulder to the unaffected side. Your physiotherapist will also palpate different areas of the shoulder complex to find the area of pain or tenderness. Further examination will involve assessment of movement and strength to establish injury to muscles or tendons.
Radiology
In addition, your physiotherapist may refer you for imaging tests to diagnosis the cause of your symptoms:
MRI: provides detailed imaging of areas injured (referred by doctors, specialists or surgeons)
Treatment
Early diagnosis and treatment of a rotator cuff tear may prevent symptoms such as loss of strength and loss of motion from setting in.
Initial treatment of rotator cuff tendinitis involves managing pain and swelling to promote healing. This can be done by:
avoiding activities that cause pain
applying cold packs to your shoulder three to four times per day
taking anti-inflammatory medications like ibuprofen and naproxen
Rehabilitation plays a critical role in both the nonsurgical and surgical treatment of a rotator cuff tear.
When a tear occurs, there is frequently atrophy of the muscles around the arm and loss of motion of the shoulder. An individualized physiotherapy program is necessary to regain strength and improve function in the shoulder.
Physical therapy
Physiotherapy will initially consist of passive exercises to help restore range of motion and ease pain.
Once the pain is under control, your physiotherapist will prescribe exercises to help regain strength in your arm and shoulder.
Steroid injection
If you have persisting symptoms, your physiotherapist may recommend a steroid injection. This is injected into the tendon to reduce inflammation, which reduces pain.
Surgery
Surgery is recommended if you have persistent pain or weakness in your shoulder that does not improve with nonsurgical treatment. In which case, your physiotherapist will refer you to surgeon for an opinion of surgical intervention.
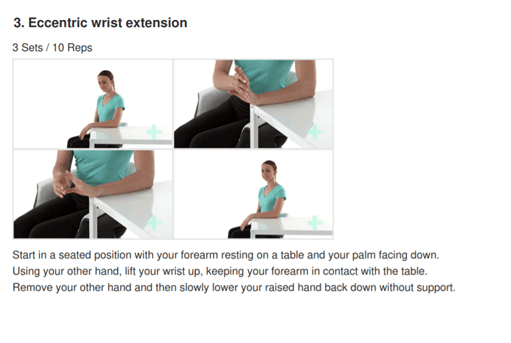
Exercises
Range of movement exercise
Pendulums
Lean forward with one arm hanging freely. Use your unaffected arm to brace against a chair for support.
With your affected side, gently swing the hanging arm from side to side, forward and back, and in a circular motion for 15-20 seconds each direction.
Slowly return to a standing position.
Repeat 4-5 times a day
Shoulder pulley (Flexion)
Put a chair against the door and sit so you are facing away from the door.
Grasp the door pulley handles with both hands.
Pull down on the pulley with your unaffected arm. This will lift your injured arm up over your head. Pull it as high as you can.
DO NOT FORCE THE MOVEMENT. Your affected arm should be relaxed. The unaffected arm does the work.
Hold for 5 seconds. Relax and repeat 10-15 times, 3 sets.
Three times a day.
Shoulder pulley (Abduction)
Put a chair against the door and sit so you are facing away from the door.
Using door pulleys slowly pull down with your unaffected arm so that your affected arm raises up and to the side without effort.
Your affected arm should be relaxed. The unaffected arm does the work.
Hold for 5 seconds. Relax and repeat 10-15 times, 3 sets.
Three times a day.
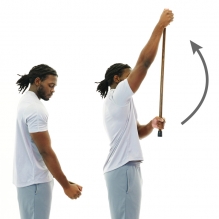
Wand flexion
Stand upright and hold a stick in both hands
Cup the top end of stick with affected hand
Using your unaffected arm hold the stick midway and drive the affected arm forward and up.
Ensure your elbow is straight throughout
Hold for 5 seconds and return to the starting position.
Repeat 10 times.
Wand Abduction
Stand upright and hold a stick in both hands
Cup the top end of stick with affected hand
Using your unaffected arm hold the stick midway and drive the affected to the side as high as able.
Ensure your elbow is straight throughout.
Hold for 5 seconds and return to the starting position.
Repeat 10 times.
Strengthening exercises with band
Flexion
Stand on one end of the band while holding the other end with your affected side.
Whilst keeping your elbow straight, lift the band up to 90 degrees to shoulder level.
Hold at the top for 1-2 seconds then lower slowly to starting position.
Attach the resistance band to a secure anchor at belly button height.
Stand with unaffected arm perpendicular to the anchor.
Place a towel between your elbow and your torso to stabilize your elbow
Grab the band using your affected side and then slow pull the band away from your body by squeezing your shoulder blade in towards the middle of your back.
Here are definitions of common terms for body parts you may hear your doctor or physio use!
Ligaments
Ligaments are cordlike extensions that serve to connect ends of two bones to form a joint. They are made up of strong, durable, slightly elastic bandlike structures comprised of collagen fibres. The structural make up of ligaments is advantageous providing joint stability by limiting excessive movement.
Tendons
Similar to ligaments, tendons contain densely packed bundles of tough collagen fibres that hold muscles together to the bone. They are located at the ends of every muscle in the human body. Bound together in tight sheaths they are made to withstand tension and transmit forces exerted by the muscle to the bone to cause movement.
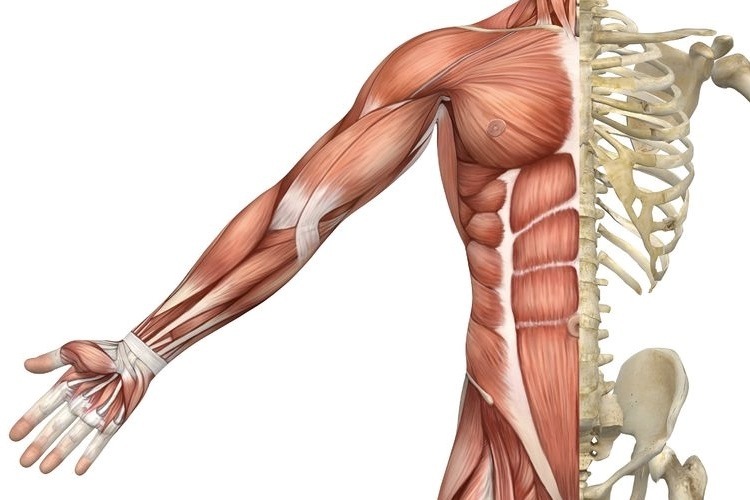
Muscles
Human body is made up of over 600 muscles categorised into three different types – cardiac, smooth and skeletal muscle.
Cardiac muscle – is only found in the walls of the heart. Its contractions help propel blood through the blood vessels to all part of the body.
Smooth muscle – is found mainly in the lining of internal organs (except the heart) including digestive and uninary tract organs, blood vessels. Smooth muscle works to transport substances through the organs by alternately contracting and relaxing.
Skeletal muscles – Skeletal muscles are the most abundant type of muscles that form the flesh of the body. They are attached to bones of the skeleton by tendons. They are responsible for voluntary movements of body. Facial expression, mobility, postural control and breathing are some of the movements we observe when skeletal muscles are subjected to voluntary control.
Bones
Skeletal system of the human body is made up of 206 bones. Bones are most involved in providing an architectural framework by providing body shape, support and protection of vital organs and for locomotion. Besides these functions, bone is a reservoir for mineral and fats as a source of stored energy and formation of blood cells. Bones are classified by their shape as long, short, flat and irregular. They are connected by ligaments to form joints.
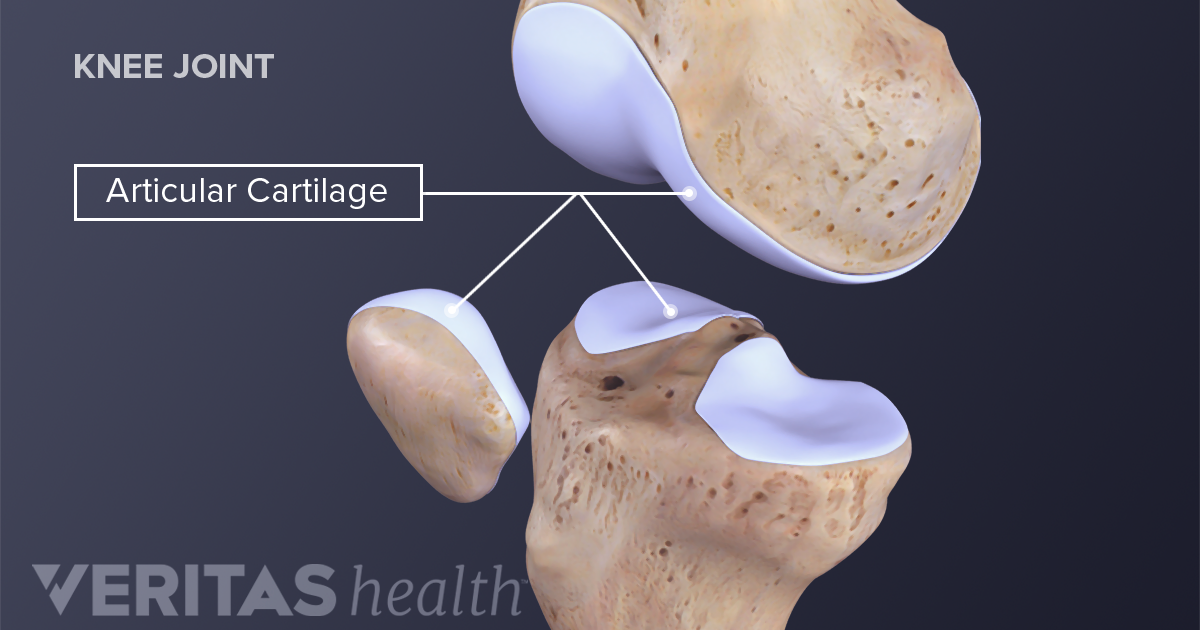
Cartilage
There are three different types of cartilage found in the human body – hyaline, elastic and fibrocartilage. Hyaline cartilage is the most common cartilage in the human body. It covers the ends of most bones at movable joints, connects ribs to the breastbone, forms the voice-box and nasal passages. It consists of high water content that provides resilience to withstand great compressive forces found predominantly in joints.