Sometimes surgery may be necessary to enhance your health and it can be stressful, both physically and emotionally. Our highly skilled physiotherapists will endeavor to actively work with your surgeon and yourself to make sure you are getting the best possible treatment towards regaining optimal function, movement, and strength both before and/or after surgery.
Elective Pre-Surgery Physiotherapy
Research has clearly illustrated the advantages of physiotherapy before elective orthopedic surgeries. We recommend pre-surgery physiotherapy to enable an enhanced healing and recovery process. Following a comprehensive assessment, you will be given a pre-surgery exercise program to keep up your strength, movement, and function, in addition to preparing you for your post-surgery programme.
Post-Surgery Physiotherapy
Physiotherapy after orthopedic surgery is essential for optimal recovery. Our skilled physiotherapists are experts at providing rehabilitation for patients after surgery and will undertake a comprehensive assessment after your surgery, which will involve ongoing evaluation of your function, mobility, and strength. As per the different stages of healing, your goals and progress, your physiotherapist will prescribe a personalized rehabilitation program. We will continue to keep close contact with your specialist as needed for the duration of your treatment.
Common surgeries requiring post-operative physio
Many surgeries, particularly those resulting from sporting injury, require physiotherapy treatment during the recovery phase.
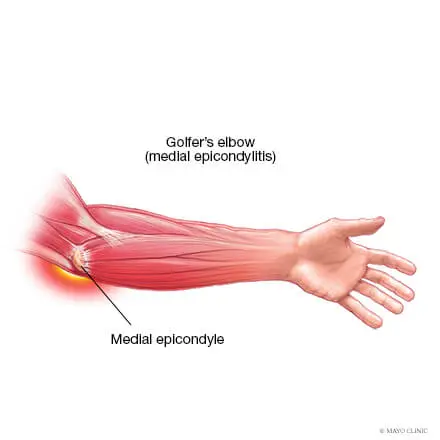
Medial elbow pain is also known as medial epicondylitis or golfer’s elbow. It is typically associated with pain on the inside (medial side) of your elbow and can spread into your forearm and wrist. This pain is the result of overloading and damage to the tendons that flex your wrist towards your palm.
Causes
This condition is triggered by damage to tendons and muscles which control your fingers and wrist. This damage is associated with excessive or repeated stresses- particularly repetitive and forceful finger and wrist movements, incorrect lifting, hitting and throwing techniques, lack of warmups and/or poor muscle conditioning.
Key risk factors for developing medial elbow pain may include smoking, obesity, being of in age bracket of 40 years old and over and undertaking repetitive activity with your arms for at least two hours daily. High risk occupations may include chefs, office desk workers, plumbers, construction workers, painters, butchers and assembly line workers. Those who partake in sports such as golf, racket sports, rowing, weight lifting and baseball are also at a higher risk.
Symptoms
Symptoms may be triggered suddenly due to a traumatic incident or may gradually develop over time and include but are not limited to:
Tenderness and pain is typically felt on the inner side of your elbow (particularly on the bony knob), and may refer along the inner side of your forearm and down to your wrist and fingers. It often worsens with certain movements. For example, bending your wrist towards your palm against resistance, or when squeezing a rubber ball.
You may feel stiffness in your elbow, and making a fist may hurt
You may experience weakness in your forearm, wrist and hand
You may experience tingling and numbness that can radiate into one or more fingers — typically to your ring and little fingers.
Diagnosis
This condition is typically diagnosed based on your medical and occupation history and a physical exam by your doctor or physiotherapist. To evaluate stiffness, strength and pain, your clinician may apply pressure to the impacted region and get you to move your elbow, wrist and fingers in various ways. You may also be referred on for imaging such as X-rays and Ultrasounds to aid diagnosis.
Management
A mix of non-surgical treatment options are effective for the majority of medial elbow pain cases, and self-resolves over time. You should rest your elbow and painful activities should be avoided. But it is very vital to maintain gentle movements of the forearm, elbow, and wrist through its range of motion.
Potential treatment options include:
Ice
Rest
Physiotherapy and acupuncture
Anti-inflammatory medications as recommended by your doctor or pharmacist
The use of a wrist and forearm brace or splint to support and rest your forearm
As your initial elbow pain lessens, your muscles around the elbow, forearm and wrist should be safely strengthened and stretched under guidance of a physiotherapist. Your physiotherapist will advise you on particular exercises, give you appropriate symptom management advice and take you through a personalised graduated rehabilitation program. If you continue to experience pain after 6-8 weeks of treatment, your physiotherapist can refer you back to your doctors, to consider administration of a cortisone injection into the elbow to help reduce pain and inflammation, and further referral onto see a specialist to seek guidance on other treatment options.
Prevention
Having a good comprehension of risk of injury and being conscious of your everyday activities may aid in the prevention of medial elbow pain. You should:
Adopt appropriate technique and form when undertaking repetitive activities or sporting motions
Keep up with adequate wrist, forearm, and shoulder muscle strength
Undertake gentle wrist and forearm stretches pre and post activities
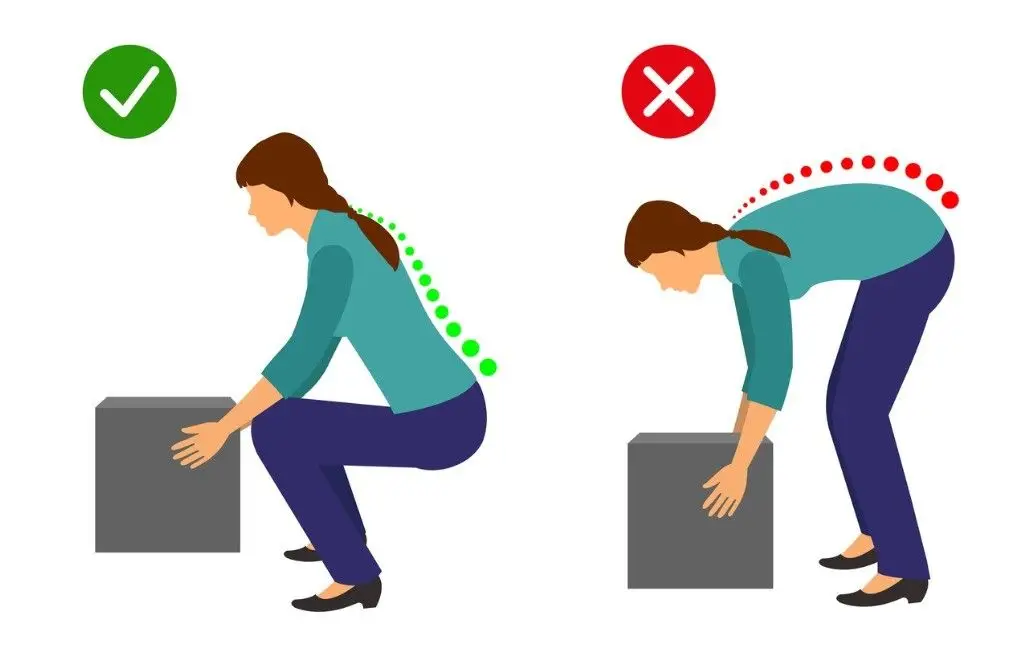
Adopt appropriate posture and body mechanics when lifting heavy objects to reduce joint strain- especially if doing so repetitively
Whether you are squatting racks of weights in the gym or squatting down to the floor to play with your children or simply squatting to sit in a chair – you are still squatting.
Truth of the matter is, squatting is more than just an exercise. If you think about it, it is a functional movement we all do many times in the day.
Knee pain from squatting is a common compliant. Although it is common, it doesn’t mean it is normal.
More often than not, the problem doesn’t only lie at the knee joint. We have to understand the complexity of our body in how our knees are directly linked with how your hips and ankles are moving. So, the purpose of this blog is not only to help you understand the basic mechanics involved in the legs when you squat, but also to help you perfect your lifting craft in the gym.
A bit on what is a squat?
Squatting is characterized as a ‘compound movement’ – fancy fitness lingo that simply means, multiple joints and muscles are moving and working in harmony to contribute to the very movement of squatting.
So here is a checklist to help you find the missing links.
Squatting check list
1. Foot arches
Feet are the foundation to our body. From a balance perspective we can go as far to say that steady the feet, steady the rest of the body. So, what happens at our feet is extremely important to consider when we talking about knee pain in general, let alone, knee pain when squatting.
Foot stability can be best explained using the analogy of a ‘tripod’. As tripod has 3 points of contact with the ground, so should our feet ideally.
The three points of a contact, as in a tripod looks like this in our feet.
Ball of the big toe
Ball of the 5th toe
Heel
Keeping this in mind, lets assess the foundation of your body – Your feet with this small exercise.
Take your shoes and socks off. Stand up tall, plant both your feet flat on the ground. Take a look at both sides individually. What do you see?
Either of your feet collapse in?
Are either of your arches diminished?
Take note of it. Next, remain standing and focus on what you feel at sole of your feet.
Think about the 3 points of contact – the tripod.
Do you feel you have evenly distributed pressure?
Take note.
Now stand on one leg – think about the same TWO things the arch and the pressures.
Which way did your foot go?
Which points of contact in the foot had more pressure?
Did your toes 3-5th lose contact from ground?
If your foot caved in and the last 3-5th toes lost ground contact, then your foot pressure is likely to sit between big toe, the base of 2-3rd toes and heel, suggesting you have a narrowed base of support. This will force the knee, hip and the rest of your body to follow in the direction, creating risk of building up unwanted pressures in others areas of your body. Before you know it, unwanted pressure results in inflammation and pain.
It is important that you consider this of high value and practice on pressure control and arch control before your look at the overall picture of squatting.
2. Ankle mobility
Your foot and ankle are closely linked – between them there are 28 bones, many muscles, ligaments and connective tissue. These anatomical structures work together to provide stability and mobility of the joints – considered KEY essentials to squatting.
Too much or too little flexibility in the ankle can be a problem. In most cases, ankle injuries result in stiffness, a hinderance to simple functional movements.
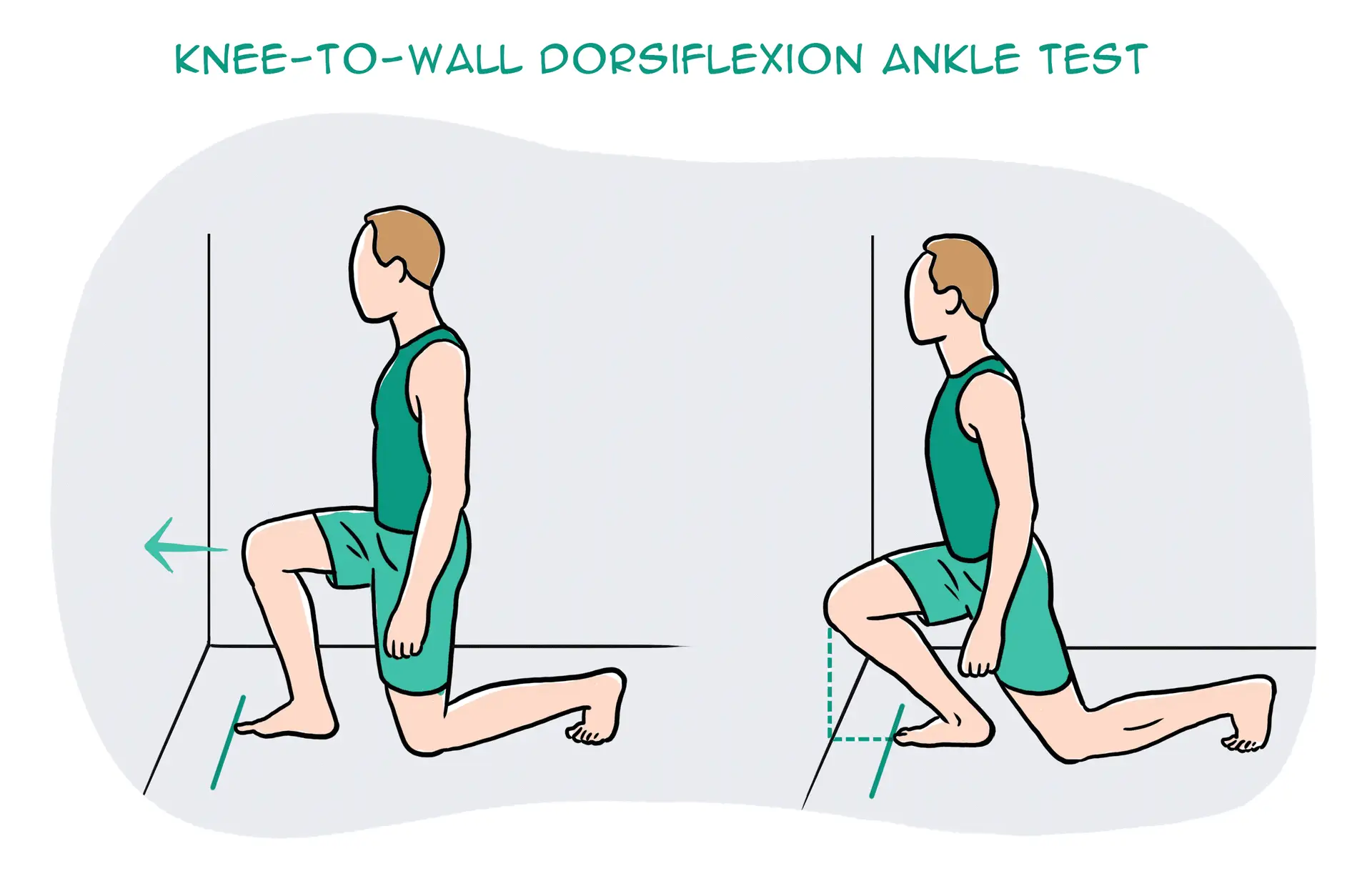
So, let’s take a closer look at your ankle with a simple mobility test.
Kneel down in front of a wall. Signal a thumbs up and measure the width of it from the wall and mark it. Place your foot on the line and drive your knee forward to the wall. Make sure you drive your knee straight forward without caving in or twisting in with your hips.
What do you see?
Can you touch your knee to the wall?
What about the other side?
Consider what you feel.
One side feels almost effortless, the other side doesn’t?
It is not uncommon to notice that the unaffected side may not be as flexible as you thought.
This is point to note – you have just discovered a link and a potential cause of your knee pain.
You need focus on stretching the muscles of your leg in a way that similar to ‘squatting’ – here is a good one!
Box ankle stretch
Use a box or a chair, plant your foot flat and rock forwards until you feel a stretch in the calf and ankle. Remember to make sure your knee doesn’t cave in or your body doesn’t twist. Do this for 20-25 repetitions, 2-3 sets. Re-test yourself.
3. Hips
Your feet are directly tied to your hips. So, the action of your hip and feet should be working together for good purposeful movement.
Here is a quick way to check this yourself:
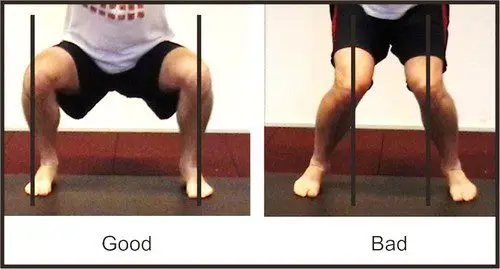
Stand tall, with your feet planted shoulder width apart. Drive your knees out to the side. You will notice your foot arch lifts.
It might be a very small amount, but worth taking note. Because, this is no different when you are squatting. If your knees collapse in, it may mean that you are not recruiting the key muscles of your hips that prevent the knees collapsing.
So, driving your knees out to match the alignment of your hip-ankle not only lifts the arches but begins the process of recruitment patterns of hip muscles to engage.
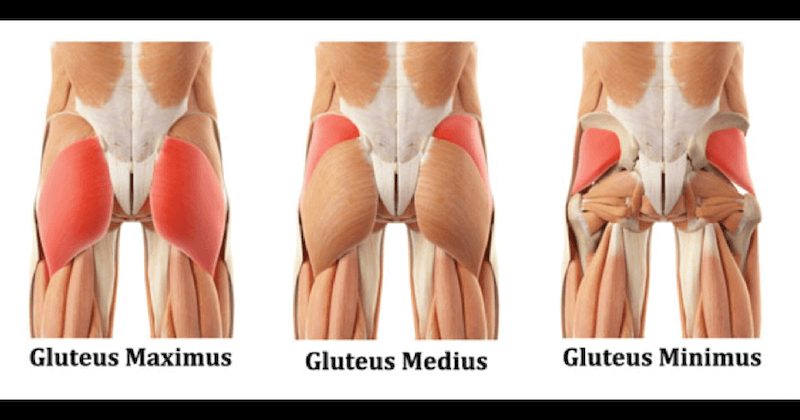
The common deficit contributing to your knee pain may be weak gluteal muscles.
Gluteal muscles are powerful muscles of the lower limb. They are a group of three muscles, each with slight different function
Gluteal maximus – hip external rotation, hip extension
Gluteal medius – hip abduction, internal and external rotation, extension
Gluteal minimus – hip abduction and internal rotation
Banded squat
Banded squats are a great way to activate your gluteus. The band not only provide resistance but provides sensory information to help you learn to push into it, therefore avoid knees from collapsing in.
If you have a lighter level resistance band, place this at knee height.
Descend in to a squat position with emphasis on pushing you knee out into the resistance band, until you reach the hip-knee-ankle alignment.
Do this 15 times, 3 sets.
For starters, work at a level that is easy for you.
Build the reps ups as you gain confidence
Weak or inadequately recruited muscles could be a result of stiffness hips.
To check your flexibility, try this next test:
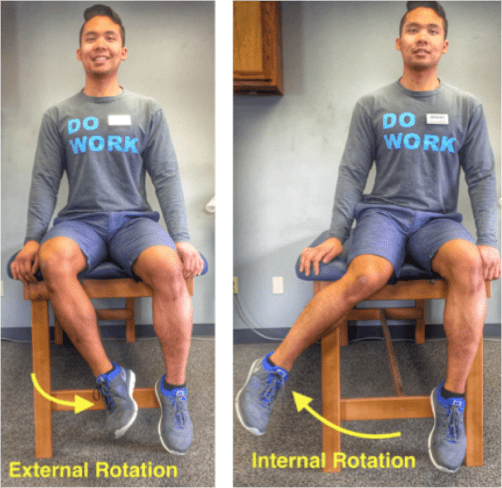
Sit on tall on a chair. Feet planted flat on ground at shoulder width apart. Test one leg at a time. Keeping your thigh in contact with the chair, drive your knee out to the side (internal rotation). Now try going inwards (external rotation).
What do you see?
Can internally rotate higher? External rotation is difficult? Or vice versa?
What do you feel?
Takes more effort going one way than the other?
Unlock the hips with this beginner hip stretch.
Sit upright on a chair. Cross one leg over on the other. You should feel a stretch in the buttock region. If not, progress by leaning forward with an upright posture. Hold for 15-20 seconds. Repeat 3-5 times.
Perfecting your squat
Perfect practice makes perfect. Now bearing the rules of movement in mind, practice your squats.
Some tips to help you better practice:
Do not worry about the depth of your squat
It’s the quality not the quantity. So as you begin to learn and adapt these principles, only squat down to a level where you feel in control of your foot, ankle, knee and hip.
Use a mirror
Visual learning is a great tool! It provides for a greater ability to correct your mistakes and perfect that ‘quality over quantity’ rule.
Start with barefoot
This allows you to connect the sensory receptors in the soles of your feet to the ground, making it much easier to learn the tripod grip.
Still having pain?
Remember, the complexity of our body and the complexity in how we move as whole can be the result of your knee pain. So, if you are still having pain – its time you get it checked.
There can be multiple reasons why your knees sound like popping popcorns or grating stones when you squat.
Generally popping in the knees is attributed to stiffness of the quadriceps muscle and the fascia that surrounds the knee joint. Overtime, stiffness causes pressure to build up under knee cap, which on movement can cause a sudden release causing a ‘popping’ sound. As worrying as it may be, most of the time popping noises in the knee without pain is NORMAL. However, for others the noise can be accompanied with a grinding sensation under the knee cap which is painful. This suggests there is an underlying pathology that needs to be addressed.
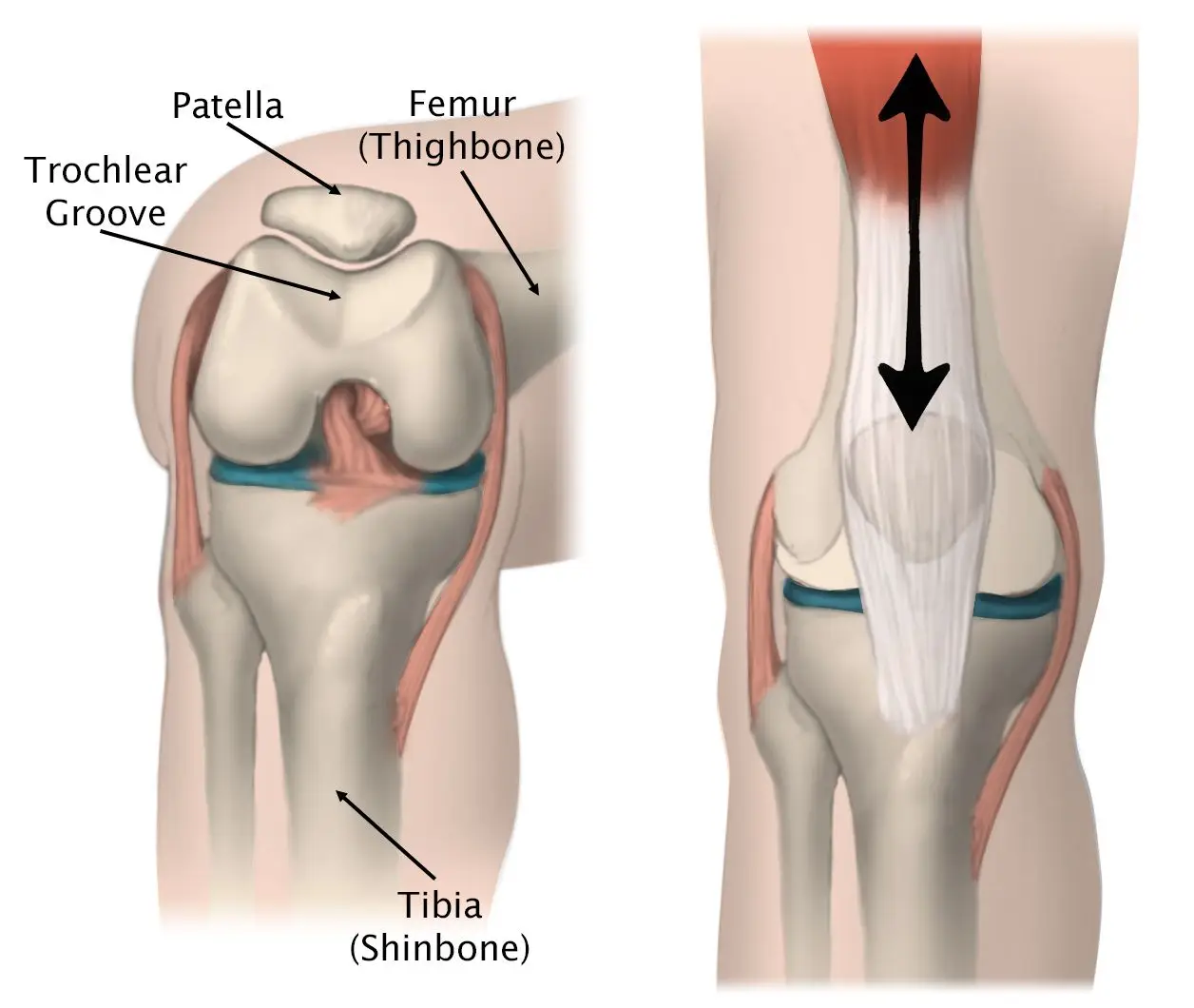
This is something we would clinically consider to be Patella Femoral Pain Syndrome aka Runner’s knee – an umbrella term that encompasses the idea of dysfunctional knee cap tracking.
When you straighten and bend your knee, naturally your knee cap tracks up and down between its groove (trochlea groove) – like a train moving up and down a train track.
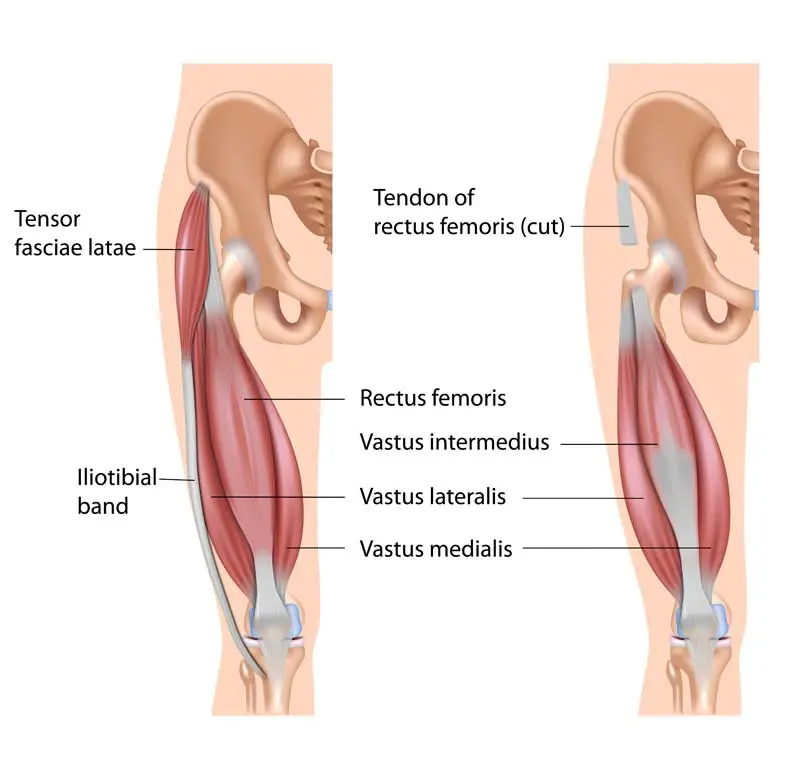
When the quadricep muscles on the outside (vastus lateralis) and inside (vastus medialis oblique) part of the leg are working in synchronization as they should, your knee cap is able to track up and down properly. However, if the quadriceps muscle (Vastus lateralis) is overly activated and the fascia (Iliotibial band & lateral retinaculum) on the outer part of you knee cap is excessively stiff, the knee cap gets pulled to the outside.
Essentially the train is being pulled and tilted more to the outside. Eventually overtime, repetitive or violent lateral pull of the knee cap increases friction in the knee grating the smooth underside of the knee cap called, chondromalacia. Additionally, the constant pulling and stiffness of the lateral side will cause stretching on the inside of muscles. On top of that, pain and swelling will cause the muscles in the inside of the leg to shut down.
Here are two steps to managing your symptoms.
STEP ONE
Foam roller or tennis ball
Instructions:
Lie on your front and place the foam roller underneath your leg.
Bend the opposite leg and bring it out to the side to help you move back and forth.
Roll the entire length of the thigh muscle, staying off the knee joint.
Make sure you move through the length of the muscle close to the knee cap as you can. You should be looking for stiff spots in the muscles and any sore spots you feel concentrate on it for couple of seconds and work deeper in to the tissue. You should also move in the inside and outside of the quadriceps muscles. Do this with you knee straight and then move into knee flexed position to optimize the release.
For a more concentrated release, use a tennis ball or a lacrosse ball especially at the quadriceps tendon where much of the stiffness is likely present. The reduced surface area of the ball allows you to work on specific spots a lot better to break down deeper areas of stiffness and create more mobility.
Do this mobility routine for 1-2 minutes
Quadricep stretches
Start in a standing position. Use support if required for balance.
Raise one leg behind you grabbing hold of your ankle, or your lower leg.
Lift and hold for 20-30 second, and then repeat for the other leg.
Get into a lunge position with back leg flat on floor
Bend your knee and slowly pull your leg into a stretch
Hold this stretch for 20-30 seconds
For comfort place a rolled face towel under the knee cap
Modified quadricep stretch
For some people if kneeling down is irritating for the knee you can modify the stretch.
Rest your leg on the chair with your foot against the back rest
Make sure your stance leg is far enough in front of the chair
Lunge forward until stretch is felt
Do this for 20-30 seconds.
NOTE: Long duration stretches of over a minute and more can decrease the potential for you to create strength and power in those muscles during your workout. So, prior to your workout focus on short duration stretches.
Functional mobility stretch
Deep squat sits are great to expand the stretch. If your symptoms are not aggravated, try deep squat sits for 30 seconds up to a minute.
Stand with feet shoulder width apart
Point your feet out to about 45 degrees
Sit in to a deep squat keeping the pressure evenly distributed across feet
STEP TWO
Now that you’ve resolved the stiffness in the lateral portion of your knee, next step is to address the muscles imbalances caused by pain and swelling. That is, turning back the firing of the quadriceps muscles.
An effective way to address this, is by doing what we call close chain exercises – these are exercises done where your feet are on the ground, such as squats. Initially you want start slow and high. Mini squats are great because they allow you to strengthen your quadriceps without putting too much compressive forces into your knee. As you get comfortable, advance to a deeper squat and slowly begin to work towards building you strength by adding on weight.
Mini bodyweight squats
Stand behind a chair or table and place your hands onto the back rest.
Keeping your back straight, bend both knees into a semi-squatting position, allowing your hands to slide forwards.
Your hips should travel backwards as you counterbalance by leaning your chest forwards.
Push through your buttock and thigh muscles as you return to standing, and repeat.
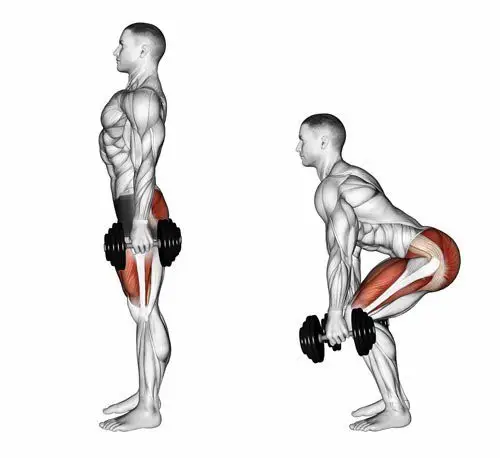
Deep bodyweight squats
Hold on to the dumbbell, keeping it close to your chest.
Step your feet wide apart and turn the toes out slightly.
Drop down into a deep squat position, keeping your feet on the floor.
Control the movement back to the start position.
Caution: Avoid deep squats especially if you have ongoing grinding pain. Do not push in to pain, as this will only increase the forces and worsen your symptoms. At this point, it is highly recommended that you come in to see a physiotherapist to examine a potential underlying pathology.
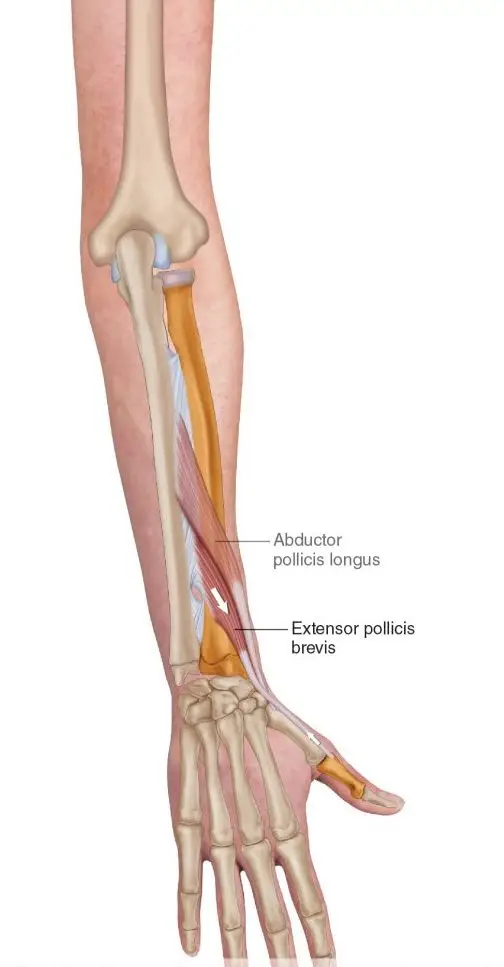
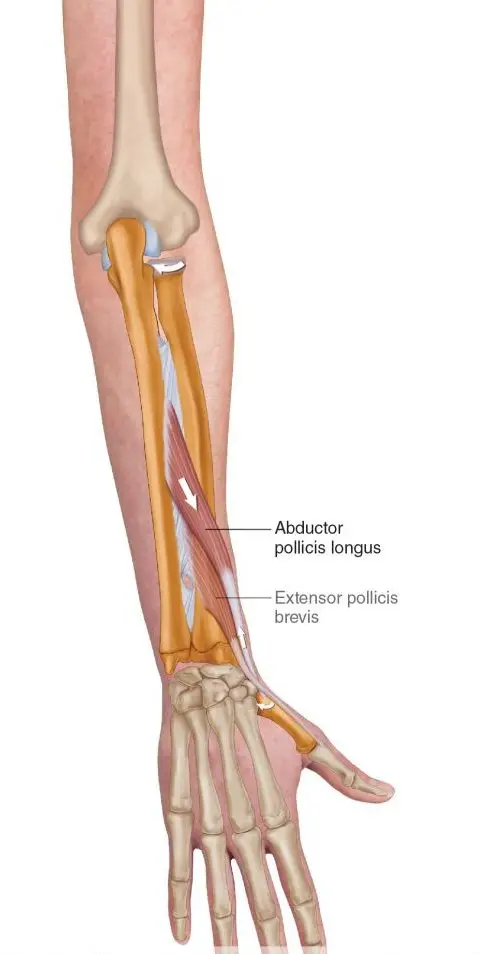
De Quervains tenosynovitis is a painful condition caused by inflammation of two prominent tendons that are located at the wrist and thumb.
The two tendons called the Extensor pollicus brevis and Abductor pollicus longus originate from the middle of the forearm travel down towards and over the wrist to insert into the thumb. Collectively they function to extend the thumb, whilst abductor pollicus longus extends and also abducts the thumb (lifting thumb up to the ceiling).
What causes it?
The most common cause of De Quervains tenosynovitis is the repetitive overuse of thumb and wrist whether it is occupational or hobby related. For example, the repetitive thumb movement whilst using scissors by hair dressers, landscapers using shears or whilst gardening). Trauma to the tendons from injuries to the wrist or the thumb can cause inflammation of the tendons.
In some cases, age related degeneration of the tendon sheath or underlying conditions such as rheumatoid arthritis increases the risk of the developing De Quervains tenosynovitis. Hormonal changes resulting in fluid build up in young mothers can commonly result in De Quervains tenosynovitis.
Symptoms
Commonly your symptoms may include:
Pain located at base of your thumb
Pain elicited by movement of thumb (gripping or making a fist)
Grating or snapping feeling
Tightness in the wrist
Swelling surrounding the base of thumb and wrist
How is De Quervains tenosynovitis diagnosed?
Your doctor or physiotherapist will be able to diagnose the condition based on your symptoms and after doing a thorough movement assessment to rule out any other potential diagnosis.
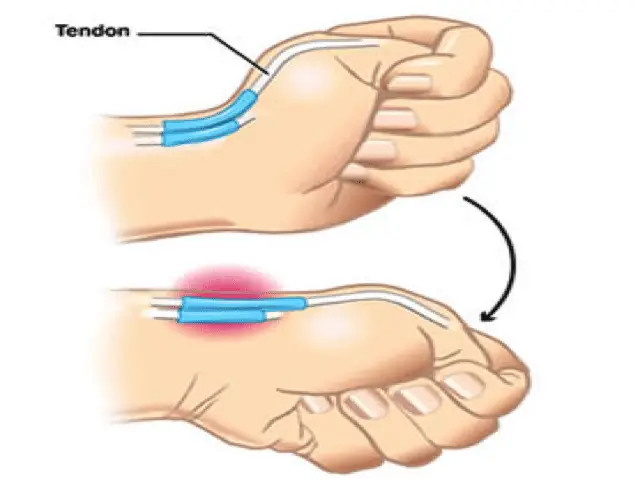
Finkelstein test is used to elicit symptoms to confirm De Quervains tenosynovitis.
How to test:
Wrap your thumb with your fingers.
Slowly bend your wrist down
A positive test would elicit pain at the site of the two tendons.
Radiological investigations in lights of ultrasound and an x-ray might be recommended for further investigations, particularly to confirm clinical diagnosis or to rule out any other possible causes of De Quervains such as osteoarthritis.
What treatment options are available?
Conservative (non-surgical) management
Conservative management measures are generally recommended as the first line of management for mild to moderate symptoms. This is because up to 60-70% of symptoms are likely to improve over a period of 6-8 weeks of regular physiotherapy intervention. In this period, the following strategies are recommended by your therapist to fast-track your recovery
Rest and application of heat or cold packs
Avoid repetitive use of thumb
Pain medications (anti-inflammatory medications) such as diclofenac or ibuprofen
Splints or braces
Steroid injection
Surgical management
In more severe cases when conservative management has failed, surgery may be recommended by an orthopaedic specialist or surgeon.
Prior to your surgery you will have the opportunity to thoroughly discuss with your surgeon the details of the surgical procedure and about the post operative rehabilitation process.
Surgical procedure
Surgery may be performed under general or local anaesthesia. A small incision is made at the wrist and thumb region. The covering of the tendons (sheath) is then separated and expanded to provide the tendon space to allow the tendon to move smoothly within the sheath. After this the, the incision in then sutured with a firm dressing applied over the suture site.
While you recover from the surgery, an information sheet with post operative guidelines will be provided to you by your surgical team. It is important that you must follow the guidelines recommended by your surgeon for optimal recovery.
In most cases your will have a follow up with your surgeon few weeks after your surgery to check your wound healing and your progress. You are often times referred to physiotherapy for strength and conditioning of your wrist and hand movements to facilitate your recovery.
RSI is typically defined as an overuse disorder- a gradual build-up of overload to nerves, tendons, and muscles arising from repetitive movements or activities. Repetitive use of the same motions leads to inflammation and damage to these soft tissues. This disorder mostly affects the upper limb- particularly the elbows, hands and wrists.
Causes
Possible causes of RSI include but are not limited to:
Undertaking the same and repetitive movements and stressing the same muscle groups
Working in cold environments
Assuming a sustained and/or awkward posture for prolonged periods of time
Undertaking a particular activity for prolonged periods of time with no rest-breaks
Frequent and prolonged use of vibrating equipment
Adopting poor postures from working at inappropriately designed workstations
Undertaking a motion which involves carrying and/or lifting heavy items
Symptoms
RSI leads to a gradual development of a broad variety of symptoms, which range from mild to severe in severity. RSI particularly affects the muscles and joints of your wrists, hands, elbows, forearms, shoulders, neck. Having said this, RSI can affect other areas of the body as well.
Common symptoms may include:
Pain
Tingling
Cramping
Increased sensitivity to heat and cold
Tenderness
Fatigue
Loss of strength
Throbbing
Soreness
Achiness
Stiffness
Struggling with typical activities of daily living, such as gripping and twisting motions, carrying light weights, writing, kitchen prepping, dressing, personal cares etc
You may develop these symptoms when you undertake a task repetitively for a period of time, and can settle when you stop. Symptoms may settle over a few hours or over the course of a few days. However, if left untreated or is poorly managed, a minor RSI may gradually progress to a nasty chronic injury.
Diagnosis
If you experience mild discomfort whilst completing particular activities at home or at your job, it is a good idea to see your GP or physiotherapist to talk about RSI. But an RSI is not always simple to diagnose as there is no particular clinical test for it. Your GP will enquire about your medical history, occupation and work environment, and other activities to attempt to identify any repetitive motions you undertake that may be the cause of your symptoms. A physical examination will be undertaken, where they will assess your movement, check for pain, inflammation, sensation, tenderness, strength and reflexes in the impacted body part. RSI may be triggered by specific health disorders like bursitis, carpal tunnel, tigger finger, ganglion cyst, or tendonitis (inflammation in your tendons). Your GP can refer you on further diagnostic tests such as X-rays, Ultrasounds, blood tests, MRIs, nerve conduction tests etc, to determine if these underlying disorders may be the cause of your symptoms. You may be also be referred onto a physiotherapist and acupuncturist for conservative treatment and management for mild-moderate issues. If symptoms persist, you will then be referred onto a specialist.
Management
Initial treatment options for the management of RSI symptoms is conservative. This includes:
Rest, Ice, Compression, and Elevation (RICE principles)
Taking regular breaks between tasks and looking after your posture
Undertaking your activities and movements with appropriate form and posture
Intake of Nonsteroidal anti-inflammatory drugs (NSAIDs), both oral and topical as prescribed by the GP
Use of cold and heat to the impacted area
Administration of steroid injections into inflamed joints and tendons
Tailored exercise prescription from physiotherapists to correct posture and strengthen and stretch affected muscles
Acupuncture
Stress reduction and relaxation training
Use of splints and braces to help protect and rest the affected muscles and tendons
Ergonomically appropriate adjustments to your workstation and work environment may be recommended by your physio and GP- for example resetting your desk and chair if you’re working at computer, and alterations to your equipment and activities/motions to lessen the strain and stress on your muscles and joints. Surgery may be necessary in some cases.
Prevention
Minimizing repetitive actions particularly if they involve the use of heavy machinery or vibration. Improving your working posture and work-environment as well a taking regular breaks. Employers often undertake risk-assessments when you join a company to determine that the work area is ergonomically fit, comfortable and appropriate for you. You may be able to request for an assessment if you have not had one or are having issues with your work environment
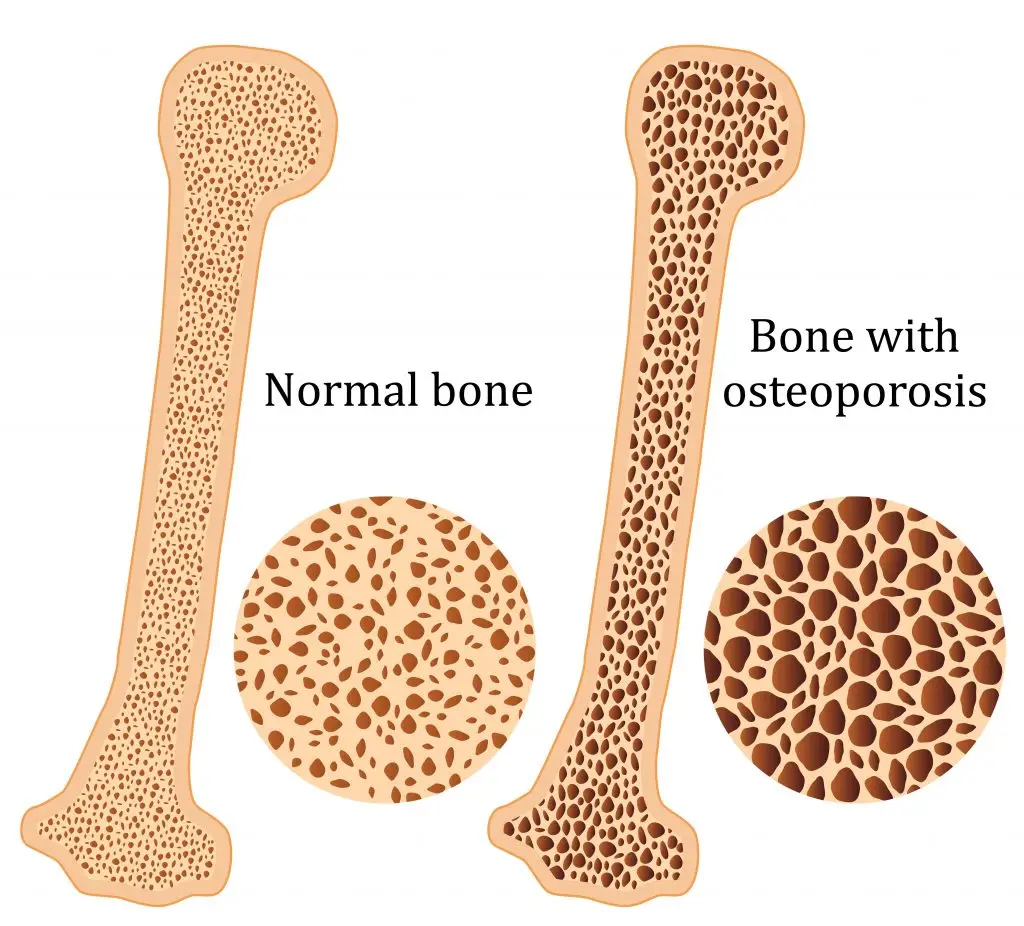
Osteoporosis is a condition which results in weak and brittle bones- to such degree that a fall or even mild stresses like coughing or bending over may result in a fracture. Bones are living tissues which are continually being broken down and replaced. However, your bones become osteoporotic when the formation of new bone does not keep up with the loss of old bone. This condition typically develops over time without any pain or other major symptoms, and is generally not diagnosed until you have sustained a fracture. The hip, pelvis, upper arm, spine and wrists are the most common structures affected by osteoporosis- related fractures.
How do you know if you have Osteoporosis?
Because there are no obvious early warning signs and symptoms, it is difficult to pre-diagnose osteoporosis. You may be unaware that you have this condition perhaps till you have one of the following:
Sustained a fracture from an incident more easily than you should have- like a simple fall or a bump
A decrease in the height of your spinal vertebrae over time
Change in posture – stooping or bending forwards
Back pain, due to a fractured or collapsed vertebra
Please see your doctor if you experience the following:
If you are over the age of 50 and have sustained a fracture
Sustained a spine, wrist, or hip for the first time
Sustained a fracture more easily than you should have (a simple fall or after a slight bump)
Risk factors
Key factors which may increase your risk of developing osteoporosis include:
Females- particularly post-menopausal Caucasian and Asian women
Over the age of 50
Excessive consumption of caffeine or alcohol
Smoking
Having a smaller or petite body frame
Poor physical activity levels and leading a very sedentary lifestyle
Family history of osteoporosis
Having low levels of vitamin D and poor dietary calcium intake
Decreasing levels of testosterone with ageing in men
Estrogen deficiency in women (irregular periods, early (before turning 40) or post-menopausal, surgical removal of the ovaries)
Use of long-term medication such as thyroid and epilepsy medications, corticosteroids
Having medical conditions such as gastrointestinal diseases; endocrine diseases; rheumatoid arthritis; cancer; and blood disorders
How will you be diagnosed?
Your doctor will review your signs and symptoms, family and medical history. You may be referred on for a specialized X-ray or CT scan to evaluate the bone density to help diagnose osteoporosis. Your bone density will be classified by comparing it to the typical bone density for a person of equivalent gender, size, and age.
How is Osteoporosis treated?
The treatment pathway chosen for the management of this condition is dependent on results of your bone density scan, gender, age, medical history and severity of the condition. Potential treatments for osteoporosis may include exercise, making positive lifestyle changes, vitamin and mineral supplements, and medications. Please consult your doctor for appropriate advice and treatment options.
How can Physiotherapy help?
Your physiotherapist will help you strengthen your bones and your muscles through a personalized and graduated rehabilitation program. Components of this rehabilitation program may include weightbearing aerobic exercises, resistance training using free weights/resistance bands/bodyweight resistance, and exercises to enhance posture, balance and body strength. Your physiotherapist will work with you to find activities that suit your needs and as per your physical activity level.
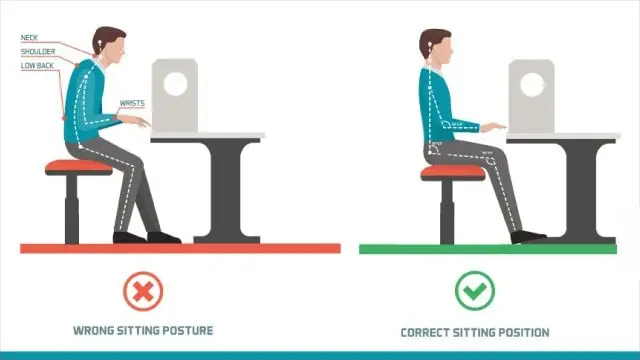
Sitting at a desk working, studying or surfing the net for long hours at a time makes it extremely difficult to maintain proper posture. That’s because our bodies are not designed for hours of idle sitting. So as the clock gets ticking many of us have the tendency lean forward, slouch our shoulders and hunch our backs.
Unfortunately, this increases pressure on multiple areas in your body. This explains why most of us experience pain and stiffness in our neck, shoulders, back and in some cases your tailbone!
So what do I need to do you ask?
The answer is simple, STAND, MOVE AND STRETCH!
It sure does sound easier said than done, especially if you are pressed with time to complete set work tasks. BUT the good news is that stretching or moving is a buildable habit that can be easily implement as you work. It doesn’t take long!
For starters set an alarm to take micro 2–3-minute break for every 20-30 minutes. Use this time to stand up, walk over to a colleague, go for a toilet break, drink water or make yourself tea or a coffee.
Or try out these simple easy stretches while you sit or stand at your desk
So let’s get started!
SPINAL TWIST:
Sit up tall, relax your shoulders
Cross one leg over the other, then place your opposite elbow on your top thigh.
Take a deep breath and as you exhale slowly twist your body (not your neck) and look over your shoulder.
Hold for 10 seconds.
Slowly return to resting position and repeat on the other side.
BACK ARCHES
Sit tall, set your feet flat on the ground hip-width apart.
Rest your hands behind your hips, then slowly arch your back as you gently tilt your head back.
If you experience pain or discomfort in your neck or tingling in your arms – do this stretch without head tilt.
Hold for 10 seconds, return to start and repeat
ARM REACHES
Sit up tall with your feet flat on the ground.
Interlace your fingers and stretch your arms straight as you turn your palms up to the ceiling.
Hold this position for 10 seconds and repeat
SHOULDER CIRCLES
Sit or stand up tall, feet hip width apart
Relax your arms and shoulder, begin by rolling your shoulder backward in a circular motion.
Do this 5 times, repeat forward circles
NECK CIRCLES
Sit or stand up tall, with feet planted flat on floor
Slowly begin to roll your head in a clockwise position
Do this 20 seconds, then repeat in a counterclockwise direction
CHEST STRETCH
Stand close to wall or a door frame
Place your forearm in a 90-degree angle at shoulder height.
Take one step forward on the leg closest to the wall and slowly rotate your chest away until you feel a stretch across your chest.
Do not hunch or round your shoulders.
Hold the stretch for 20 seconds, repeat
Do this both for both sides
BACK EXTENSIONS
Stand with your legs at hip width apart and straight.
Place your hands on your hips.
Lean your body backwards, trying to arch in the lower back as much as you can, lifting your chest up towards the ceiling.
Try to avoid allowing your hips to swing forwards too far.
Hold this position for 10 seconds, return to start position & repeat 5 times.
FLOOR REACHES
Sit on a chair with upright posture
Slowly bend forward to plant your hands on the floor.
Hold for 10 seconds, return to start
SHOULDER BLADE SQUEEZE
Start in an upright position.
Practice bringing your shoulder blades back and down.
Picture gently drawing your shoulder blades towards the centre of your lower back.
This is a subtle movement, ensure you do not over strain your shoulder blades when performing this action.
Hold for 10 seconds, repeat 3-5 times
SHOULDER BLADE STRETCH
Clasp your hands together and hold them in front of your body.
Push your arms as far forward as you can whilst rounding your shoulder blades.
Gently drop your chin down to your chest.
Hold this position while you feel a stretch between your shoulder blades.
WRIST STRETCHES
Stretch out your arm straight in front of you with your palm facing away
Use your opposite hand to gently pull your palm back
Hold for 5 seconds, repeat with your palm facing your body
Having a fall is dangerous at any age, however, they become more frequent and may most probably result in injury in adults 55 years and over. It is also estimated that in Aotearoa, approximately a third of older adults over the age of 65 sustain a fall every year. This leads to harmful consequences for them, especially for those who live alone. Alongside, sustaining serious injuries, you may face loss of independence, mobility and confidence. But!!! The good news is that there are a number of ways that you can reduce your risk of falling.
So Why Do Older Adults Have Falls?
Poor lower limb strength
Cognitive and functional impairment
Nutritional deficiencies
Prior and/or ongoing history of falls
Vision deficits
Balance or gait disorders
Medication related- especially when using anti-depressants, sedatives, anti-arrhythmics, anti-hypertensives, diuretics, and anti-convulsants
Hazards around your home environment such as loose carpets, slippery surfaces, poor lighting, lack of safety equipment particularly in the bathroom/toilet
Medical conditions such as vertigo, dizziness, diabetes, postural hypotension, drop attacks, and fainting spells
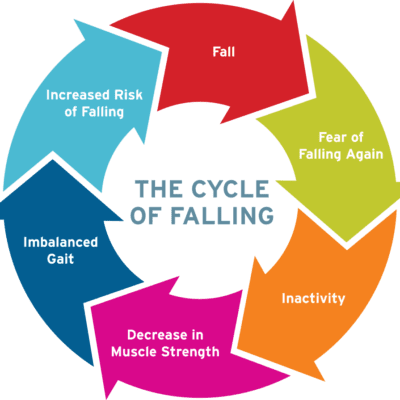
The Vicious Falls Cycle
Older adults who have had a fall may limit what they do because of their loss of self-confidence and fear of falling. Whilst this may seem like the most sensible thing for them to do, it increases their risk of falls. This is because, this leads to a further reduction in muscle strength, coordination and balance. Hence, it is healthier for older adults to keep up with their activities they enjoy as safely as they can, work on improving their muscle strength, coordination and balance, and manage their blood sugar levels, blood pressure, and weight under the guidance of their doctor.
Falls prevention tips
Below are some measures you may take to prevent yourself from falling:
Exercise regularly: A number of benefits include better sleep, improved muscle strength, balance and flexibility, increased energy levels, stronger bones, better management of weight, blood sugars and blood pressure. Exercise programs tailored especially for muscle strength and balance have resulted in a reduction in the number of falls and injuries resulting from falls by approximately 30% and 50%. It is advised that you speak to your doctor or physiotherapist before initiating or progressing your exercise levels.
Keeping your vision in check: Vision deficits makes getting around safely a lot harder. Therefore, you should get your eyes checked yearly and wear your contact lenses or glasses with the correct prescription strength.
Being aware of the effects of your medication: As they may have certain side effects that increase your risk of falls. You should review your medications with your doctor for side effects like drowsiness or dizziness.
Reduce hazards at home: Most falls typically take place at home. So be sure to make your home safer by removing tripping hazards, having adequate lighting, and adding in handrails in hallways and bathrooms/toilets.
Other tips:
Taking your time to get up and when moving around- no rushing!
Having a personal medical alarm (please talk to your doctor about how to get one)
Using a night light when you get up at night
Wearing appropriate, supportive and well-fitted shoes
Not using an easily moveable object to stabilise yourself
Using the support of handrails in bathrooms and hallways
Avoiding or being very careful on wet or slippery floors
Appropriately using your walking aids
If You Have Had a Fall
If you sustain a fall, it is vital for you to stay calm.
If you think you are able to get up safely, try to bend your knees, roll to your side, and attempt to get into a 4-point kneeling position. If there is a chair near by or if you are able to crawl towards one, you can use it as support to get yourself up. Please take your time and rest as needed.
If you are unable to get up safely, attempt to crawl or roll towards a phone. You may call out to other members in your household or your neighbour. If you’re at risk of falls, please do consider the use of a personal medical alarm to call out for help when you have a fall.
After a fall, please contact your doctor as soon as you can for an assessment of potential injuries sustained, muscle strength and balance to help prevent future falls. You may be directed to community or in-home sessions to enhance your balance and strength. Please discuss this with your doctors.
Rheumatoid arthritis (RA), a chronic inflammatory condition associated with swelling, pain, fatigue, and joint deformity. Although there are no known cures for this condition at present, a combination of treatments are available to help manage your symptoms. RA is the 2nd most common form of arthritis after osteoarthritis and is known to affect 1–2% of New Zealand’s population.
Signs and Symptoms
RA may develop very quickly or gradually over time, with its signs and symptoms, as well as the severity varying from one person to another. This condition is associated with episodes of remission and flare ups, with or without apparent triggers.
Other symptoms may include
Swollen, tender joints- (often accompanied by warmth and redness)
Joint pain
Joint stiffness which worsens in the mornings and after a period of inactivity
Fever, loss of appetite weakness, and fatigue
Muscle pain
Changes to the skin and nails
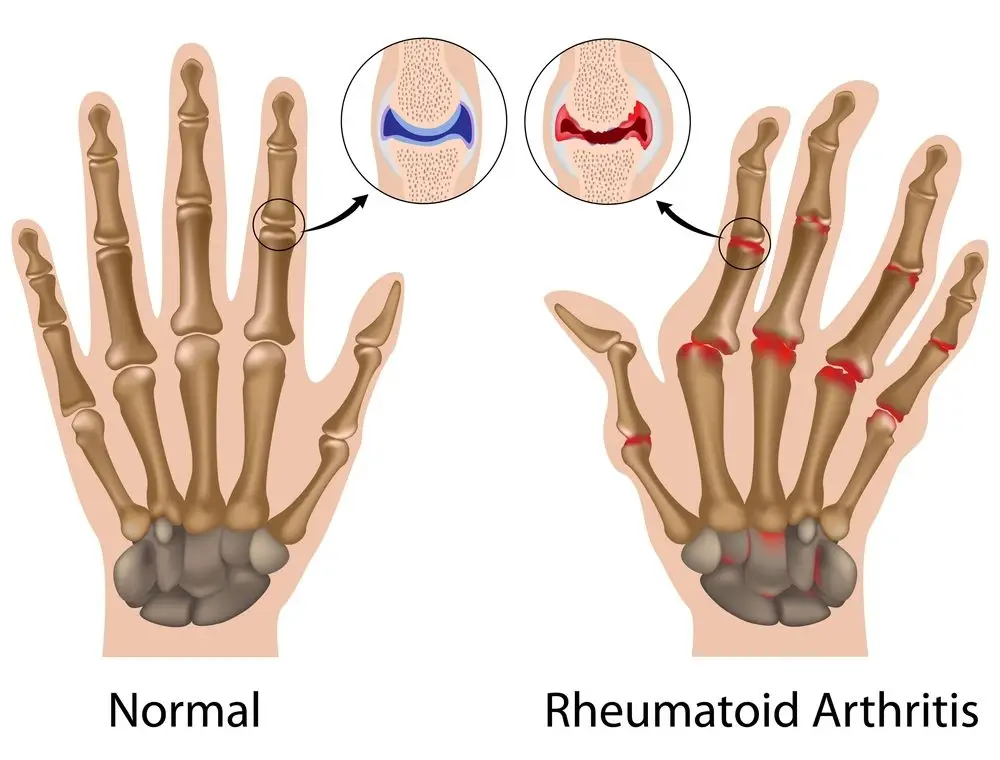
In the early stages of RA, you may notice its impact on your smaller joints- especially in your toes and fingers. And as this condition develops, your symptoms typically branch out to the bigger joints- your shoulders, ankles, knees, wrists, hips and elbows. Symptoms are likely to affect your joints bilaterally. Over time, RA also causes joints to deform and shift out of place.
Because RA is a systemic condition, it is estimated that approximately 40% of the RA population may experience symptoms and signs other body systems than the joints. These may include:
Kidneys, lungs, heart
Skin, eyes, mouth
Bone marrow
Nerves and blood vessels
Causes and Risk Factors
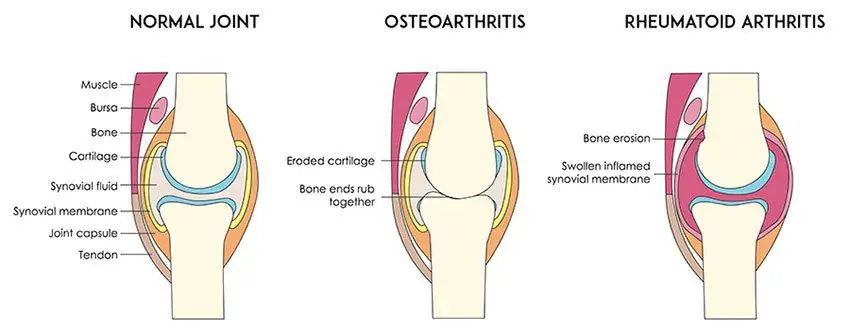
Your immune system is designed to help protect your body from infection and disease. However, in RA, changes occur in your immune system that (for poorly understood reasons), causes it to mistakenly attack the healthy soft-tissues of joints resulting in pain, swelling and inflammation. Because of this ongoing process, over time damages to the lining of your joints and other soft-tissues may lead to bone erosion and joint deformity. It can also have an impact on your heart, lungs, nerves, eyes and skin.
One can get RA at any age, although it is more probable to develop in those in the age bracket of 25-50 years old. Though rare, under 16s may also develop Juvenile RA or Still’s disease.
Risk factors for the development of RA include:
Family history of RA
Age bracket of 25-50 years old
Smoking
Women are more likely to develop RA than men
Obesity
Diagnosis
At present there is no single test to confirm a clinical RA diagnosis. It is often difficult to differentiate this condition in its initial stages from other forms of connective tissue inflammation (fibromyalgia, lupus, gout etc.).
Your doctor will get your full medical history (as well as any familial history of RA), discuss your signs and symptoms, undertake a physical assessment- particularly of your joints, and refer you on for imaging and blood tests. X-rays may help evaluate RA progression in your joints over time, whilst MRI and ultrasound imaging may help evaluate the severity of RA in your body. The blood test will evaluate your level of anti-bodies and proteins (including the rheumatoid factor protein that is present in approximately eighty percent of the RA population), and markers of inflammation.
Management
At present, though there is no cure for RA, a range of treatments are available which may help slow its’ progression and reduce pain and inflammation, minimise and/or prevent joint damage and maximise joint movement.
A combination of prescribed medication as advised by your doctor and other treatment options as noted below are recommended:
Cease smoking if you are smoker
Physiotherapy will help improve and maintain your joint range of motion, increase your muscle strength, and decrease your pain. Additionally, your physiotherapist or occupational therapist will be able to teach you ways of using your body efficiently to reduce stress on your joints
Finding a balance between rest and activity
Use of heat and cold packs to help ease pain and inflammation
The use of splints or braces for joint support as needed
Hydrotherapy- exercising in water reduces the pressure on your joints, whilst the warmth of the water will relax your muscles and help lessen your pain.
Seeking regular medical advice and check-ups to monitor your RA symptoms and the progression of the condition