Low back pain is a common health problem which affects up to 80% of the population at some stage in their life.
In New Zealand ACC spends in excess of $130 million a year treating back pain related injuries.
Most back pain occurs between the ages of 25 and 60, and most typically in the 40s.
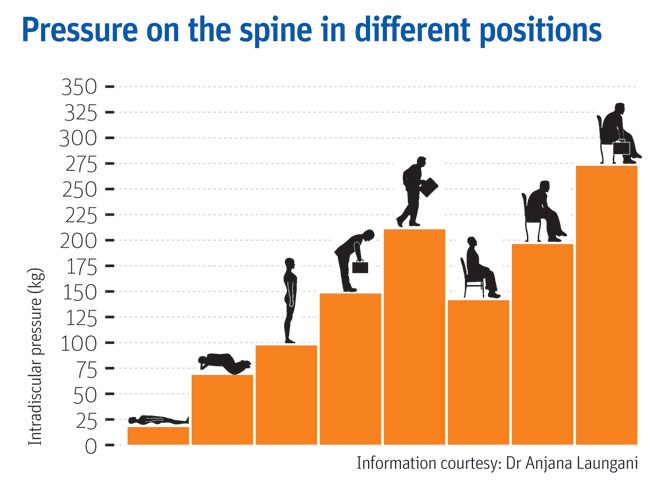
In an era of smart devices, posture has never been more important or harder to achieve. As technology continues to grow, sitting at a desk on a computer or on our phones is becoming more prevalent at work. Having a sedentary desk job can result in sitting for around 8 hours a day. This position actually increases the load on your spine more than standing. Spinal pressure “sits” around 140mm pressure. This pressure usually does not hurt the back right away however, builds up over time and can even change the structure structure of your spine. So, if you slouch then spinal pressure increases to 190mm; add some weight and you’ve put 275 pounds of pressure on your spine.
A compromised spine constricts your blood vessels and nerves, causing problems with your muscles, discs, and joints. And all of these problems can lead to headaches, fatigue, and even breathing problems. Your back is a delicate machine. When one part falls out of alignment, it can affect everything setting off a domino effect and wreak havoc throughout your back and body.
Below is a graph showing different postures and the pressure it exerts on the spine;
But, remember: While you may feel comfortable and supported in your chair and find a perfect sitting posture, staying in the same position for long periods is not healthy for your spine. Varying your postures by occasionally standing and moving around for at least a few minutes each half hour will help keep your spinal joints, muscles, tendons, and ligaments loose and pain free.
Stand Up for Your Spine
If you don’t have a sit-stand desk, you can still combat “sitting disease” and protect your spine. Consider these tips:
Do some work standing at a high table or counter.
Use a lumbar roll behind your back when sitting to improve seated posture
Set a timer on your computer for a stand-and-stretch break every 30 minutes.
Exercise to assist in improving body weight to lessen additional load on the spine
Strengthen the core to provide additional support
The focus is simple: Reduce your sitting throughout the day. But, remember that varying postures is best for your back and neck, so do not go the opposite extreme and never sit. Alternating sitting, standing and movement throughout your day is the best way you can keep your spine safe and body healthy—at work and beyond
Still having back pain?
Schedule an initial assessment with one of our Physiotherapists so they can determine the root of the problem. During this assessment your physiotherapist will be able to decide whether your pain is a source of nerve root irritation, discogenic, postural related, or musculoskeletal. After arriving with the consensus of the problem, we will be able to use many techniques to relieve the back pain. These include: manual therapy, therapeutic exercise, and postural recommendations.
To find your nearest Physio Fusion clinic and book an appointment call 09 6266186 or visit our websitehttps://physiofusion.co.nz
Headaches happen for lots of reason and can be cause by several sources- both primary and secondary. Once major “red flags” are ruled out, understanding the type of headache is important in order to have it properly addressed.
A cervicogenic headache is a secondary headache arising from a musculoskeletal dysfunction within the cervical spine, and is a disorder that many physiotherapists treat. The main players that are typically involved in generating the pain are the joints, discs, ligaments, nerves and/or muscles found in the upper portion of the neck.
Characteristics of a Cervicogenic Headache:
Pain usually one sided or one side dominant
Pain originates from the back of the neck and radiates along the forehead, orbits around the eye, temple area and ear.
Steady ache or dull, diffuse pain that travels into shoulder region
Limited neck movement especially when turning head
Tenderness to touch at the muscles at the base of the head.
Here are some exercises that would help alleviate your pain:
Cervical side flexion with chin tuck
Sit upright in a chair.
With your shoulders relaxed, relax one arm to your side.
Drop your opposite ear to your shoulder until a stretch is felt.
Using your fingers, tuck your chin in, as to resemble a double chin.
Gently release pressure with your fingers and hold this position.
Relax and repeat
2. Levator stretch Neck stretch – levator scapula
Start in a seated position.
Place the hand of the side you want to stretch down by your side.
Tilt your head forwards and to the opposite side at an angle, as if you are trying to
look at your armpit.
Keeping your back straight and upright, continue to tilt your head down until you
feel a stretch from the base of your skull down into your shoulder blade.
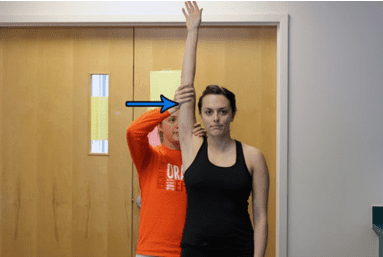
3. Neck stretching (Upper trapezius)
Stand up straight.
Take the hand on the symptomatic side and place it behind your back.
Take your other hand and place it on your head.
Tilt your ear directly down towards your shoulder and hold this position.
You should feel a stretch down the side of your neck.
If you believe you experience Cervicogenic Headaches get in touch with us https://physiofusion.co.nz/ for an in-depth assessment and lets knock out those headaches and decrease you dependence on pain meds
The restrictions and change brought by the outbreak of COVID-19 has resulted in a great deal of control being taken from our hands; this has been anxiety provoking for many of us. Nevertheless, it’s important to re-evaluate, acknowledge and place focus upon the matters that we DO have control over so that we can gain our personal power back!
Lockdown Productivity Tips
Check in with yourself: how is your body and mind feeling. Embrace your emotions and give yourself permission to feel the way toy do.
Stay connected: Social connection is inevitably limited at the moment but catching up with people via text or facetime will help prevent feelings of isolation.
Maintain some form of routine: Maintaining a routine helps provide some structure do days which often all seem to merge into one.
Get fresh air where possible: Daily fresh air can provide an easy change of scenery when we are stuck at home most of the day.
Gentle exercise is a MUST!
Stay Hydrated: Drinking enough water is important to keep your body hydrated and makes sure your body functions properly.
Eat well- You’d be surprised how your diet can affect how you feel. Gut health in particular is linked to mental health.
Get to that “thing” you’ve been delaying for months
Pick up a good book
Learn new habits or rediscover old ones
These may seem like simple strategies but sometimes it’s the simple things that are most effective
“One day this will all be over and we will be grateful for life in ways we never felt possible”
The gratitude we will have for the things we once took for granted will be unmeasurable- getting on a plane, an impromptu visit to the cinema, a shopping spree, going to the gym, even meeting a friend for lunch at a café. Keep going, nothing lasts forever and we have so much to look forward to. In the mean time take each day as it comes, be kind, support those who are struggling and keep going! You are stronger and more resilient than you know!
You may have seen videos or posts online about people talking about a specific area of your shoulder known commonly as the “Rotator Cuff” and wondered what they were on about. Your shoulders do a lot of important things you might take for granted! They help you get something off a high shelf, comb your hair, or play a game of cricket.
It’s a complicated process that your body makes look easy. And your rotator cuff is a big part of that. It protects and stabilizes your shoulder joint and lets you move your arms over your head. It’s importance is widely used in sports like swimming, tennis and netball.
In New Zealand healthcare, shoulder injuries have one of the highest prevalence when it comes to ACC claims and overall cost. Within this, rotator cuff injuries are among the most common pathologies affecting New Zealanders. Other pathologies include acromioclavicular injuries, dislocations, osteoarthritis and frozen shoulder.
So, what exactly is the cuff and how does it influence the shoulder?
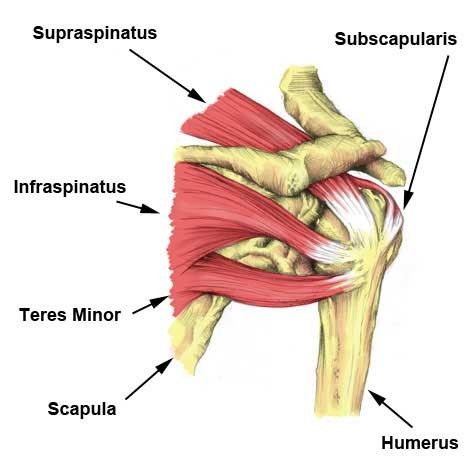
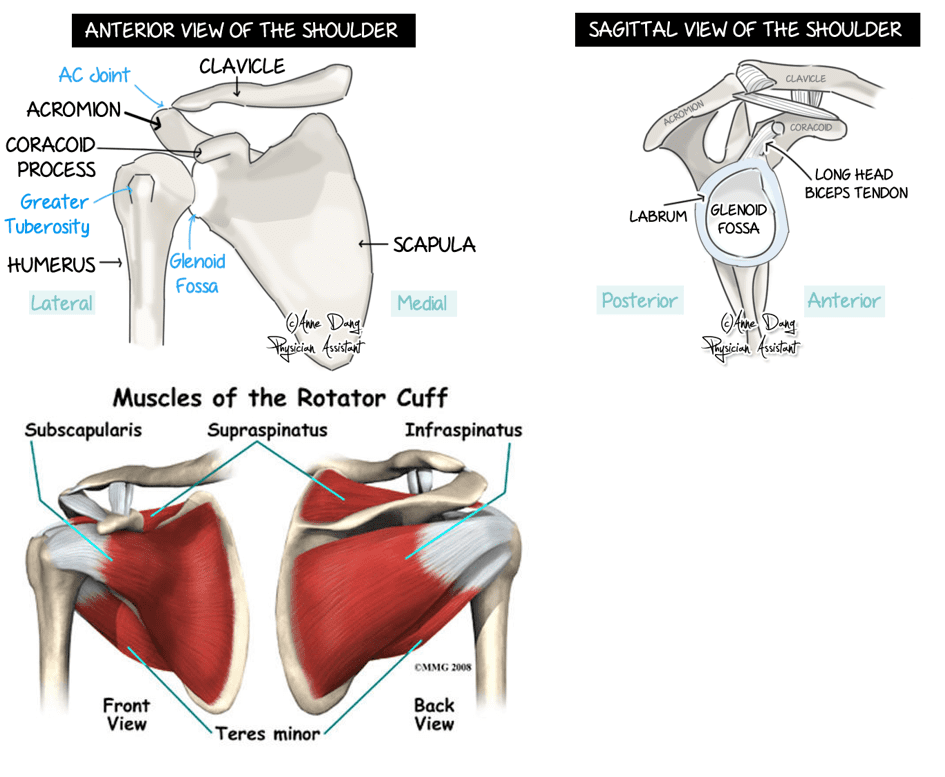
The rotator cuff (RC) is a combination of four muscles that run through and attach onto specific areas of the humeral head (top of the arm bone).
Supraspinatus, Infraspinatus, Teres minor and Subscapularis are the four muscles comprising the RC and each one plays an important role however they all contribute to shoulder stability:
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
A thin triangular muscle that helps perform abduction
A thicker, triangular muscle that performs external rotation.
The smallest muscle of the cuff, helps with rotation as well
The largest muscle of the cuff performs internal rotation (arm behind your back!)
Many people suffer from shoulder pain, so here are the most common injuries that can happen at the rotator cuff:
Rotator Cuff Tear:
A rotator cuff tear is often the result of high levels of load over a short amount of time or a high impact force stressing one or more of the tendons/muscles. Fortunately, majority of tears are partial. Tears are more common in people with jobs that involve heavy loading or lifting or in high impact sports like rugby. It also can happen suddenly if you fall on your arm or try to lift something heavy. Common and easily treatable with conservative management by a physiotherapist, a rotator cuff tear can come right.
Rotator Cuff Tendinopathy:
A rotator cuff tendinopathy is the most common shoulder pain complaint/injury resulting in inflammation and irritation of one or more of the cuff tendons. This pathology is more common in individuals who have an occupation where repetitive use of the shoulder, particularly in an overhead position such as carpenters or painters, or individuals that play highly repetitive, throwing sports like tennis, baseball or volleyball. Once again, this injury is treatable by a physiotherapist, conservative management can be very effective in treating these injuries with a thorough, well planned exercise program to help get patients back to doing what they love.
Majority of people experience pain around the shoulder joint, with some movements being highly provocative. Tenderness on touch at the affected site is also common – this helps your physiotherapist hone in on potentially which tendon is causing those problems!
Medical management vs Physio management
Medical management will be advised by your local GP if you decide to see them first. They might prescribe NSAIDs (anti-inflammatory medications such as ibuprofen) to help with the pain you’re experiencing and recommend you see a physiotherapist. Depending on your injury as well as your ability to function, surgery may be an option if conservative medical and physio treatments don’t help. Most people get by without the need of surgery but some tears can be too large to heal without the use of surgical intervention.
Physiotherapy management is designed around reducing pain and disability, restoring range of motion and helping people return to work or sports to perform how they were prior to the injury. In the early stages of these injuries, rest and ice and/or heat are recommended to allow the inflammation to settle – then your physiotherapist will begin to introduce a detailed exercise program, this may include:
Isometric (static hold) exercises
Resisted movements using bands
Range of motion exercises to restore lost movement
Functional loading – task specific or sport specific
If this is successful, the last step is to build back up the strength that was lost over time – this is done by concentrically (against gravity) loading the affected tendons/muscles in a way that they adapt and lay down more tissue, grow and becoming stronger in hopes that you get to return to what you enjoy!
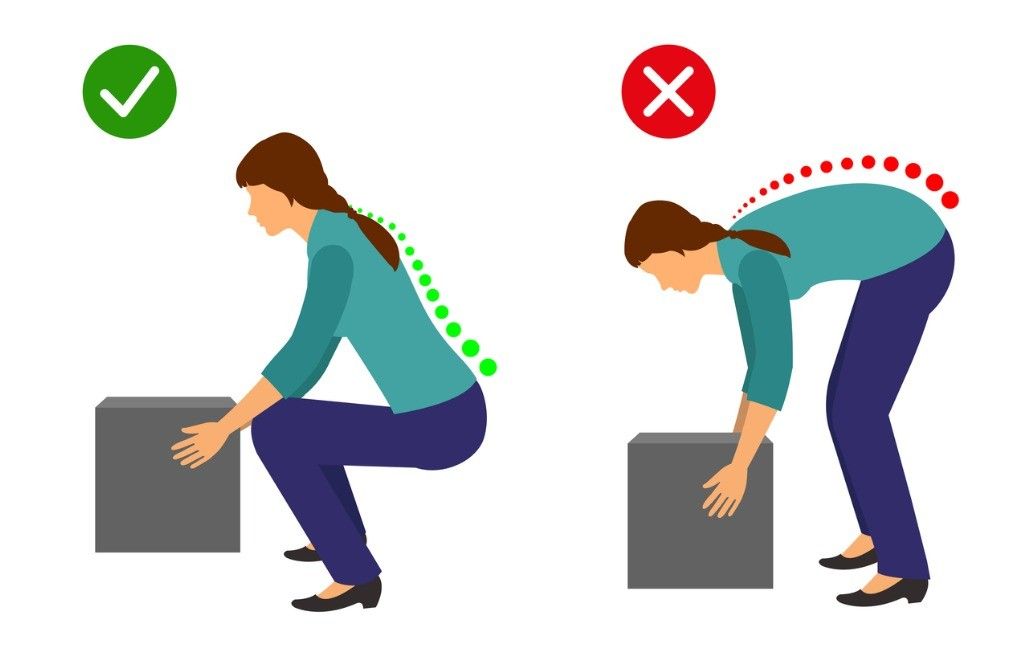
One common belief about lifting is that rounding your back when lifting an object is considered dangerous while lifting with a straight back is considered safe…
However, there is a lot of misinformation circulating around lifting mechanics and what is deemed “good technique” versus “bad technique.”
Here are some key myths and misinformation that you may have heard:
A ROUNDED BACK WHILE LIFTING OVER STRESSES THE BACK MUSCLES AND LIGAMENTS
Research has shown that regardless of lifting position, whether you’re stooped, squatting or weightlifting, your back has to produce the same amount of force. Statistically speaking, it’s not significantly different.
FLEXING THE SPINE WHILE LIFTING INCREASES THE LOAD ON THE LUMBAR DISCS
Under heavy loads, discs are unlikely to fail unless >95% flexion is achieved (which is near impossible)
With low loads, the disc is unlikely to fail unless you do thousands of repetitions continuously
Your body is an amazing adapter, this includes discs! Your discs can adapt and become more and more able to handle loads when stressed appropriately
THESE COMPOUND TO CAUSE INJURIES AND PAIN TO THE BACK MUSCLES AND DISCS
Resistance training has demonstrated through countless studies the ability to increase bone mineral density (BMD) of the lumbar spine. BMD is actually positively associated with the strength of the spinal discs and ligaments at that level. With appropriate loading and training, disc, ligament, bone and muscles are going to adapt favourably
A NEUTRAL SPINE IS SAFER, STRONGER, MORE EFFICIENT AND BETTER TO LIFT WITH
There is no significant difference between activities that encourage more spinal flexion and one’s that do not in the long term
Lifting with lumbar flexion is not a risk factor for low back pain
Research has shown lifting with a bent back is more metabolically and neuromuscularly efficient
When the spine is in extension during bent over activities, the hip is actually flexed to a greater degree – decreasing the ability for the glutes and hamstrings to create as much internal torque. Flexing the spine reduces this effect and reduces the moment arm for the hip extensors
STOP BACK PAIN & INJURIES BY LIFTING WITH A NEUTRAL SPINE
Your lumbar spine flexes every time your hip flexes! It is impossible to isolate one versus the other. It is also impossible to not flex while doing common movements
Extreme flexion however (>/=100%), may pose an increased risk under heavy loads, but not at light loads
You may still be wondering why you have back pain (stay tuned for our next blog!). Your pain may not be directly related to your lifting strategy.
Could you have pain with forward bending? Absolutely.
Is bending at the lumbar spine an increased risk for pain or injury? In the vast majority of situations, no.
If I have pain with forward bending, is it bad to temporarily limit doing so? Not at all.
Should I fear bending at the spine with or without pain or injury? No. Being fearful of flexing/moving your spine is actually a stronger predictor of disability and back pain.
Work on moving through your spine, after all it’s what it is designed to do! Choose comfortable movements and gain confidence over time, then build up your strength gradually with resistance training – try and not to push too fast, we want nice, healthy adaptation! Give your body time to adapt, back pain is not quick fix sometimes but you are resilient and with healthy, normal movements and some patience, you will be okay.
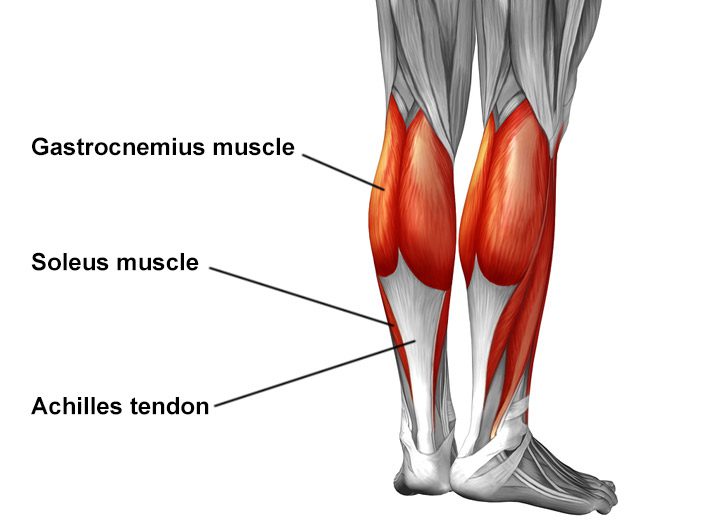
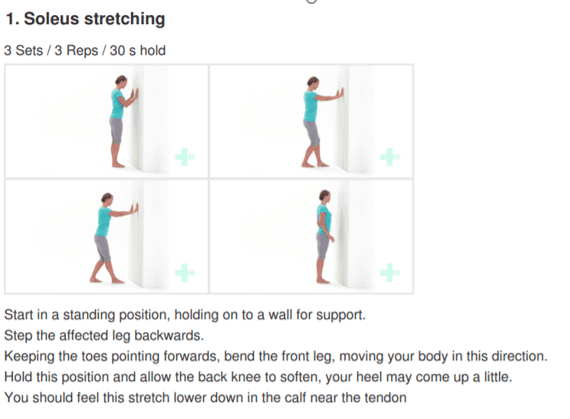
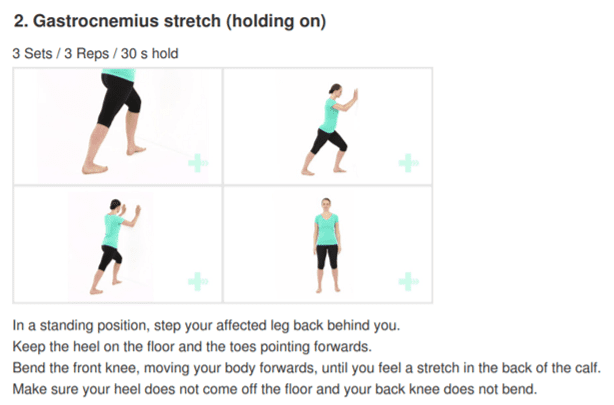
The Achilles tendon is the largest tendon in the human-body. It is a band of tissue that connects your calf muscles to your heel bone (calcaneus). This tendon primarily facilitates general mobility such as walking, running, climbing stairs, jumping, and standing on your tip toes, by helping to raise the heel off the ground.
Common Achilles Pathology
Achilles tendinitis and tendinosis are two common disorders and are typically classified as overuse injuries.
Achilles tendonitis involves inflammation of the Achilles tendon. Inflammation is the body’s natural response to injury or disease, and often causes swelling, pain, or irritation. This inflammation is typically short-lived. Over time, if this is left resolved, the condition may progress to degeneration of the tendon- Achilles tendinosis, in which case, the tendon loses its organized structure and is likely to develop microscopic tears.
There are two types of Achilles tendonitis and it is based on which part of the tendon is inflamed:
Insertional Achilles tendonitis affects the lower portion of your tendon where it attaches to your heel bone.
Non-insertional Achilles tendonitis involves fibres in the middle portion of the tendon and tends to affect younger people who are active.
In both non-insertional and insertional Achilles tendinitis, damaged tendon fibres may also calcify (harden) and often bone spurs (extra bone growth) develop with insertional Achilles tendinitis. Achilles tendonitis may also increase your risk of sustaining an Achilles tendon rupture (tear).
Causes
Typically referred to as “overuse” conditions, Achilles tendonitis and tendinosis are often caused by the sudden increase in repetitive activity involving the Achilles tendon. This can put too much stress on the tendon too quickly, that can then lead to micro-injury of the tendon fibres. Because of this ongoing stress on the Achilles, the body is not able to repair the injured tissue. The structure of this tendon is then modified, resulting in continued pain and other symptoms. The Achilles tendon also has poor blood supply that makes it more susceptible to injury and may make recovery from injury slow.
Common factors that may lead to the development of disorders of the Achilles tendon include:
Weak and/or tight calf muscles
Rapidly increasing the amount or intensity of exercise within a short span of time
Hill climbing or stair climbing exercises
Presence of bony spurs in the back of your heel
Changes in footwear – especially changing from wearing high-heeled shoes to flat shoes
Wearing poor fitting, inappropriate, or worn out shoes during sporting activities
Exercising without adequate warm-ups and stretching
A sudden sharp movement which causes the calf muscles to contract and the stress on the Achilles tendon to be increased. This can cause the tendon fibres to tear.
Excessive mobility
Poor feet positioning and biomechanics (excessive pronation and flattening of the arches of the foot)
Symptoms
Common symptoms include:
Pain and stiffness along the Achilles tendon especially first thing in the morning
Pain along the tendon or back of the heel that worsens with activity
Severe pain the day after exercising
Visible thickening of the tendon
Tenderness to touch
Bone spur
Swelling that is present all the time and gets worse throughout the day with activity
If you have experienced a sudden “pop” in the back of your calf or heel, you may have torn your Achilles tendon. Please seek urgent medical attention if you think you may have torn your tendon.
Diagnosis
If Achilles tendonitis or tendinosis is suspected, please deter from any activity or exercise which causes the pain. It is advisable to see your doctor or physiotherapist as soon as possible so that an accurate diagnosis may be made and appropriate treatment recommended.
You will be asked about the nature and duration of your symptoms and the medical professional assessing you will have a look at your foot and ankle. Ultrasound scanning may be used to evaluate the damage to the tendon and/or surrounding structures.
An MRI may be recommended if symptoms persist. X-rays may also be taken to rule out other disorders which may cause symptoms like Achilles tendonitis and tendinosis.
Treatment
Treatment will depend on the nature, severity, and length of the injury. Generally speaking, the longer the symptoms are present before treatment commences, the longer the timeframe until full recovery is attained. Full recovery may take between three and nine months.
Initial treatment options in the early stages may include:
Rest – to avoid further injury to the area
Ice – to reduce inflammation
Elevation – to reduce swelling
Non-steroidal anti-inflammatory drugs to reduce pain and inflammation.
How physiotherapy can help:
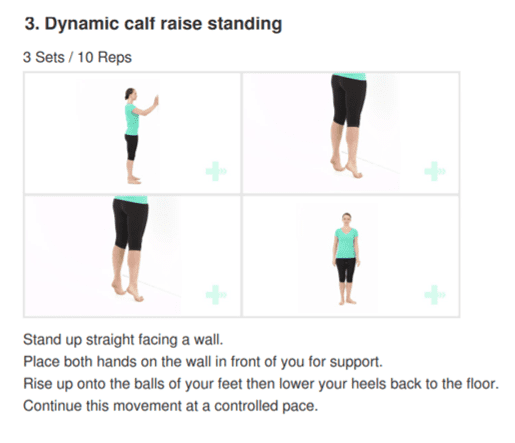
Physiotherapy typically focuses on two main areas: treatment and rehabilitation. Treatment may entail massage, shockwave therapy, acupuncture, gait re-education, and gentle stretching, whereas, rehabilitation predominantly entails strengthening of the Achilles and surrounding musculature.
Strengthening of the muscles surrounding the Achilles tendon facilitates healing in the tendon itself. Strengthening is attained through the utilization of specific exercises, that will be taught by your physiotherapist. It is common for the rehabilitation programme to take up to three months.
Myth 1: When you see a physiotherapist you just lie on the bed and get given an ice or heat pack.
At Physio Fusion we use an active approach to treatments. Physiotherapy will include manual hands-on therapy to facilitate tissue healing and tissue load tolerance alongside an exercise program individualized to your needs.
Myth 2: If I have elbow pain then the injury must be in my elbow.
The area of pain is not always the area that is the issue! It may be a result of a previous injury that was never fully rehabilitated. This is where we can help you out. Our assessment will consist of gathering information on your presenting complaint, any previous injuries or traumas (physical and emotional) and a medical history followed by an objective evaluation of your body. This allows us to get to the root cause of the pain and manage your symptoms most effectively.
Myth 3: I can’t do any of my normal activities while I attend physiotherapy.
Not true! Our Physiotherapists want to keep you as functional as possible whilst allowing your injury to heal. During the initial assessment your physiotherapist will determine what activities you can do and advise you on those that must be avoided. You will then be given clear and timely objectives to ensure you reach your goals to get you back doing what you love!
Myth 4: A scan will show me exactly what is wrong.
Sometimes it will, but sometimes it won’t. It’s no secret that our bodies change as we age, so even people without pain are likely to have an imperfect scan. Medical imaging can sometimes play an important role in the assessment and management of your musculoskeletal issue. When necessary, your physiotherapist will know what type of imaging to refer you for.
Myth 5: Is cracking my back/neck/knuckles bad for me?
There is no strong evidence to suggest that ‘cracking’ your joints causes degeneration, laxity or instability. The ‘cracking’ occurs when we move a joint to its end range. The audible sound happens because of ‘cavitation’ in the joint; this involves gas bubbles popping within the fluid surrounding the joint as pressures change.
But is it good to crack?
Self manipulation can be a helpful way to reduce the feeling of stiffness or tightness. If you are finding that you need to ‘crack your joints’ often it is good to know that there are many other more beneficial ways to provide greater long term relief.
Top tips:
Ask your physiotherapist to provide you with some specific exercises to help you overcome the feeling of stiffness or tightness.
Move regularly and avoid movements or positions that exacerbate your symptoms until you have been seen by your physiotherapist.
This is a common phrase people use to describe a physiotherapists role. It is true that as a profession we like to work ‘hands on’. This is because our profession is directly affiliated with the anatomy of our clients and by using touch we can more accurately assess, locate and treat any dysfunctional motions within your body. Our physiotherapists like to use massage as it is a great way reduce pain and improve bodily function but their skill set is much more extensive than this.
Did you know?
There are well over 20 different treatment approaches commonly used by physiotherapists. These may include, but are not limited to:
Exercise prescription.
Joint mobilization.
Joint manipulation.
Instrument mobilization.
Muscle energy techniques (improves muscle and joint function).
Neurodynamics (mobilization of the nervous system).
Taping.
Dry needling.
Acupuncture.
Myth 2: Always sit up straight! Slouching is bad.
In fact, forcing yourself to adhere to the traditional ‘good posture’ (back straight and shoulders back) may be putting unnecessary tension on your body. That isn’t to say being upright is bad either, but in life we must always find a balance. To reduce stress on your body whilst seated, ensure your back is supported and your feet firmly on the ground. To prevent and reduce the likelihood of back pain we must look to vary our posture frequently throughout the day and ensure we take short breaks to stretch, stand and walk.
Myth 3: Physiotherapy sessions are painful
Physiotherapists aim to help you reduce pain and get you back to doing what you love! Whether your injury is acute or chronic our physios always ensure they work within your pain threshold to help you regain lost movement and function.
Myth 4: I need a referral to see a Physiotherapist’
We have got you covered!
Remember, physios are registered health care professionals. Physio Fusion is a registered ACC provider. This means that if you have had a recent injury (within one year), you can see us directly and we can help you lodge an injury claim directly with ACC. You do not need a referral for your doctor.
Myth 5: Lower back pain …. surgery is my only option
Around 70-90% of the total world population will experience lower back pain during the course of a life time. Symptoms can range from mild to severe and can either last for short or long periods or remain constant. Back pain can be very debilitating and when the pain does not resolve as soon as anticipated many fear that surgery may be the only option. In few cases surgery may be necessary, but for the majority there’s often nothing to fear, and with time and a gradual loading or exercise program, you can make a full recovery.
Did you know ?
Back pain is not always a sign of injury or damage. Each individuals back pain story will be different, and for many non-physical factors play a huge part in their story. These factors can be:
Psychological –
Stress.
Fear of movement.
Depression.
Health related –
Sleep deprivation.
Physical inactivity.
Smoking (nicotine decreases blood flow to your back).
Overweight.
Physio Fusions top recommendations for keeping back pain away:
Keep active – regular exercise nourishes joints, strengthens muscles, increases blood flow and improves your mood.
Sleep well.
Maintain a healthy weight by ensuring you maintain proper nutrition and diet.
Sit in a chair with good lower back support.
Quit smoking.
Ensure that when you lift or pick up objects you do so in a safe manner. This is something one of our physiotherapists can guide you with.
See a doctor urgently if you have the following symptoms:
Numbness in the groin or buttocks.
Loss of bladder or bowel control.
Redness or swelling on your back.
Difficulty walking.
Constant pain, especially at night.
Pain that is getting much worse, or spreading up your spine.
Numbness or pins and needles in both legs.
Feeling unwell with your back pain, such as a fever or significant sweating that wakes you from sleep.
The shoulder is made up of two joints. These are the acromioclavicular joint (collar bone meets shoulder blade) and the glenohumeral joint (upper arm meets shoulder blade). The shoulder is protected by ligaments (joining bone to bone) and muscles known as the rotator cuff. These muscles form tendons (joining muscle to bone) and play a major role is stabilising the shoulder. Under some of these muscles and tendons, there are small fluid filled sacs ((known as bursae) to allow easy gliding of muscles over bone. The upper arm also joins the shoulder blade with the help of the Labrum (soft tissue around the glenoid cavity). Finally, this is all surrounded by a fluid filled sac which lubricates the shoulder joint for better movement known as the shoulder capsule.
History taking and assessment
You can expect questions regarding the history of your shoulder injury from your physiotherapist such as:
How the injury happened
Where the pain is in your shoulder
Whether you have a ‘dead arm’ feeling
If you feel a different sensation from the other side or some weakness
Aggravating and easing activities
Past history and family history of shoulder injuries or pain
Once these questions have been asked and answered, your physiotherapist will proceed to perform an assessment of you and your shoulder. This can range from:
Posture assessment
Strength and sensation testing
Testing of ROM (movement of the shoulder)
Special testing to check joint stability, muscle integrity and possible signs of shoulder damage
Investigations
Based on your history and examination findings, your clinician will suggest the best possible investigation for you.
In most cases, initial X – rays are done to rule out broken bones.
Ultrasounds can be used to diagnose some ligament and tendon damage such as rotator cuff tears.
MRI is the best form of imaging but this does come at a higher cost and higher exposure to radiation. The MRI scan can identify bone, ligament and tendon injuries in the shoulder.
A CT scan is not usually performed in cases of the shoulder.
Possible injuries to the shoulder
Instability:
If you have dislocated your shoulder in the past or continue to experience shoulder dislocations, you may have some instability of the shoulder. Normally you may develop a “dead arm”. You may also feel a sense of heaviness, numbness or an inability to move the arm which persists for a few minutes. If you are experiencing these episodes more frequently with less force, it is advised that you see your healthcare professional.
Treatment:
Non-surgical management involves a period of rest with a parallel shoulder strengthening program for stability. This is done when the injury is acute and non-recurrent.
Surgical management is opted for when there has been damage to the ligament and Labrum as well as ongoing recurrence of shoulder dislocation. Surgery is associated with a reduced rate of recurrence.
Rotator cuff:
The four muscles that make up the rotator cuff are Supraspinatus, Infraspinatus, Teres Minor and Subscapularis. Rotator cuff injuries are one of the most common disorders of the shoulder. It is believed that most of these injuries are caused by overuse of the shoulder. Often heavy lifting, sports involving the shoulder and repetitive shoulder movements are associated with rotator cuff pathology. These injuries cause pain and stiffness with overhead activity (eg: throwing a ball or putting a shirt on) and pain is worse at night. You may also feel some weakness in your injured arm because of pain.
Treatment:
A partial thickness tear in the rotator cuff can heal with non-surgical management. These are managed with physiotherapy exercises, corticosteroid (cortisone) injections and most importantly, time. It is important to know that the pain will improve over time.
A Full thickness tear in the rotator cuff will normally be managed with surgery. This is followed by immobilisation of the arm for up to 6 weeks in a sling. After these 6 weeks, you should begin a physiotherapy program in order to aid your recovery.
Acromioclavicular joint (ACJ):
This is a fairly common injury and normally occurs in athletes involved in contact sport or when falling directly onto the point of the shoulder. You may experience some pain and swelling in the upper shoulder. This pain can sometimes occur with no reason at all and it is important to voice this to your clinician.
Treatment:
You will be treated surgically or non-surgically according to the severity of your injury.
Non-surgical management includes a brief spell of rest and sling use for protection and healing. This is followed by early mobilisation of the shoulder and a subsequent strengthening program. Your physiotherapist can also assist you with taping in order to return to activity.
Surgical management is followed by a physiotherapy program as outlined by the shoulder surgeon. This is normally done for a quicker return to play in contact sports or when pain is severe and a trial non-surgical management has not worked.
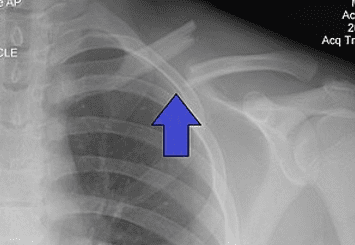
Fractures:
These normally occur as a result of direct trauma to the arm such as a fall. They can be very painful and are usually associated with a lot of swelling around the area.
Treatment:
Depending on where and how severe the injury is, the doctor may opt for surgical or non-surgical management.
In either of these cases, you will undergo a period (6 weeks maximum) of immobilisation of the upper limb to allow for healing. At the end of this period, it is important to see your physiotherapist to begin rehabilitation of your arm.
What to expect
Acute phase:
Immediately following an injury, you should be offered adequate pain relief. A sling can be very effective and can be combined with simple analgesia, anti-inflammatory medications and ice therapy.
Passive range-of-motion (ROM) exercises, including pendulum and active-assisted exercises, should be considered. You will be encouraged to maintain fitness (if comfortable) using a stationary bike or general walking.
Early Rehabilitation phase:
When your pain has settled and your ROM has improved to 60-70% of the unaffected side, you can progress with rehabilitation.
Exercises that might be useful in this phase include:
Stretch of the shoulder
Progressive ROM exercises with the goal of achieving full ROM
Strengthening of the rotator cuff and scapular stabilisers
Late Rehabilitation phase:
You will progress to this phase when you have a normal (full and painless) ROM and 75% strength of the unaffected side.
The types of exercises that might be useful in this phase include:
Progressive multi-planar exercises
The addition of further resistance exercises, including weights and the use of medicine balls and more functional activity
Plyometric exercises
Return to sport:
When you have a normal range of motion and more than 90% strength of the uninjured side, you can progress to return to sport. This should be done in a gradual manner.
A return-to-sport programme may involve:
Initial unopposed training
Opposed training in a controlled setting
Match practice
Return to sport when this full progression has occurred
In conclusion:
Your shoulder injury will be treated and tailored to you. With most shoulder injuries, physiotherapy can be helpful in operative and non-operative management.
Early management or rehabilitation of your injury could go a long way in speeding up your recovery process and avoiding re-injury in the future.