
SHIN SPLINTS NO MORE
Shin splints, medically known as medial tibial stress syndrome, is a collective term used to describe multiple conditions that cause shin pain. Therefore, it is important to establish that there is not one singular cause.

Shin splints, medically known as medial tibial stress syndrome, is a collective term used to describe multiple conditions that cause shin pain. Therefore, it is important to establish that there is not one singular cause.
Myth 1: When you see a physiotherapist you just lie on the bed and get given an ice or heat pack.

At Physio Fusion we use an active approach to treatments. Physiotherapy will include manual hands-on therapy to facilitate tissue healing and tissue load tolerance alongside an exercise program individualized to your needs.
Myth 2: If I have elbow pain then the injury must be in my elbow.

The area of pain is not always the area that is the issue! It may be a result of a previous injury that was never fully rehabilitated. This is where we can help you out. Our assessment will consist of gathering information on your presenting complaint, any previous injuries or traumas (physical and emotional) and a medical history followed by an objective evaluation of your body. This allows us to get to the root cause of the pain and manage your symptoms most effectively.
Myth 3: I can’t do any of my normal activities while I attend physiotherapy.

Not true! Our Physiotherapists want to keep you as functional as possible whilst allowing your injury to heal. During the initial assessment your physiotherapist will determine what activities you can do and advise you on those that must be avoided. You will then be given clear and timely objectives to ensure you reach your goals to get you back doing what you love!
Myth 4: A scan will show me exactly what is wrong.

Sometimes it will, but sometimes it won’t. It’s no secret that our bodies change as we age, so even people without pain are likely to have an imperfect scan. Medical imaging can sometimes play an important role in the assessment and management of your musculoskeletal issue. When necessary, your physiotherapist will know what type of imaging to refer you for.
Myth 5: Is cracking my back/neck/knuckles bad for me?

There is no strong evidence to suggest that ‘cracking’ your joints causes degeneration, laxity or instability. The ‘cracking’ occurs when we move a joint to its end range. The audible sound happens because of ‘cavitation’ in the joint; this involves gas bubbles popping within the fluid surrounding the joint as pressures change.
But is it good to crack?
Self manipulation can be a helpful way to reduce the feeling of stiffness or tightness. If you are finding that you need to ‘crack your joints’ often it is good to know that there are many other more beneficial ways to provide greater long term relief.
Top tips:

Myth 1: ‘’Physiotherapy is just massage’’

This is a common phrase people use to describe a physiotherapists role. It is true that as a profession we like to work ‘hands on’. This is because our profession is directly affiliated with the anatomy of our clients and by using touch we can more accurately assess, locate and treat any dysfunctional motions within your body. Our physiotherapists like to use massage as it is a great way reduce pain and improve bodily function but their skill set is much more extensive than this.
Did you know?
There are well over 20 different treatment approaches commonly used by physiotherapists. These may include, but are not limited to:
Myth 2: Always sit up straight! Slouching is bad.

In fact, forcing yourself to adhere to the traditional ‘good posture’ (back straight and shoulders back) may be putting unnecessary tension on your body. That isn’t to say being upright is bad either, but in life we must always find a balance. To reduce stress on your body whilst seated, ensure your back is supported and your feet firmly on the ground. To prevent and reduce the likelihood of back pain we must look to vary our posture frequently throughout the day and ensure we take short breaks to stretch, stand and walk.
Myth 3: Physiotherapy sessions are painful
Physiotherapists aim to help you reduce pain and get you back to doing what you love! Whether your injury is acute or chronic our physios always ensure they work within your pain threshold to help you regain lost movement and function.

Myth 4: I need a referral to see a Physiotherapist’
We have got you covered!
Remember, physios are registered health care professionals. Physio Fusion is a registered ACC provider. This means that if you have had a recent injury (within one year), you can see us directly and we can help you lodge an injury claim directly with ACC. You do not need a referral for your doctor.
Myth 5: Lower back pain …. surgery is my only option

Around 70-90% of the total world population will experience lower back pain during the course of a life time. Symptoms can range from mild to severe and can either last for short or long periods or remain constant. Back pain can be very debilitating and when the pain does not resolve as soon as anticipated many fear that surgery may be the only option. In few cases surgery may be necessary, but for the majority there’s often nothing to fear, and with time and a gradual loading or exercise program, you can make a full recovery.
Did you know ?
Back pain is not always a sign of injury or damage. Each individuals back pain story will be different, and for many non-physical factors play a huge part in their story. These factors can be:
Psychological –
Health related –
Physio Fusions top recommendations for keeping back pain away:
See a doctor urgently if you have the following symptoms:

It is scientifically proven that physical exercise is one of the greatest rehabilitation methods. Numerous studies consistently prove the indisputable benefits of exercise therapy.
Did you know?
People who are physically active for approximately seven hours a week are 40% less likely of dying early than people who are only active for less than 30 minutes a week.

So what are the health benefits of exercise?
Any many many more!!
So what is stopping you?

Time – Time waits for no one. But there is plenty of it in the week to make a difference. Don’t fear moving slowly forward, fear standing still.
Knowledge – Starting is always the hardest part! Here at Physio Fusion we are always willing to help guide and advise you on all aspects of your physical health. We are very fortunate to have good connections with other healthcare providers who can also help to assist you!
Confidence – You have our vote! At physio fusion we embrace the lifestyle we promote. We are here to facilitate your needs and to guide and advise you on all aspects of your health.
Cost – Your health is your wealth. At Physio Fusion we provide the highest quality treatment and advice at very affordable prices.We have special rates for clients with a Gold Card (no co-payment) or Community Services Card ($10.00).
Distance – For those of you unable to travel to our clinics, or who are isolating currently due to COVID-19 we have you covered! We offer telehealth (online video) consultations, supported with a rehab exercise programme tailored to your needs via the online database Physitrack.
Secure your appointment today by booking online or phone us on:
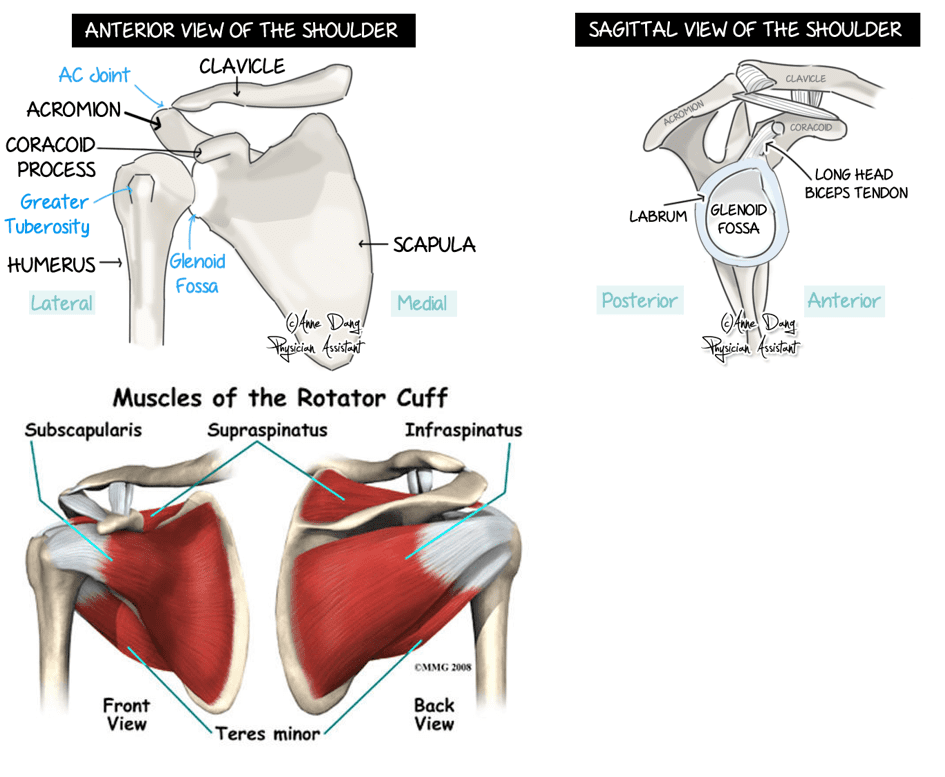
The shoulder is made up of two joints. These are the acromioclavicular joint (collar bone meets shoulder blade) and the glenohumeral joint (upper arm meets shoulder blade). The shoulder is protected by ligaments (joining bone to bone) and muscles known as the rotator cuff. These muscles form tendons (joining muscle to bone) and play a major role is stabilising the shoulder. Under some of these muscles and tendons, there are small fluid filled sacs ((known as bursae) to allow easy gliding of muscles over bone. The upper arm also joins the shoulder blade with the help of the Labrum (soft tissue around the glenoid cavity). Finally, this is all surrounded by a fluid filled sac which lubricates the shoulder joint for better movement known as the shoulder capsule.
You can expect questions regarding the history of your shoulder injury from your physiotherapist such as:
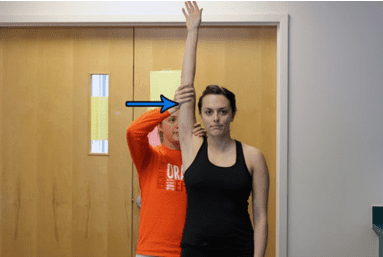
Once these questions have been asked and answered, your physiotherapist will proceed to perform an assessment of you and your shoulder. This can range from:
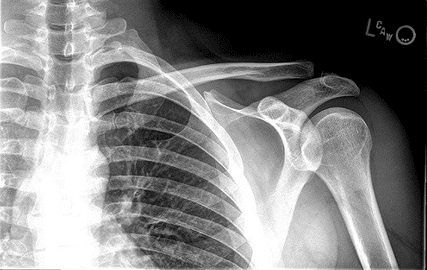
Based on your history and examination findings, your clinician will suggest the best possible investigation for you.
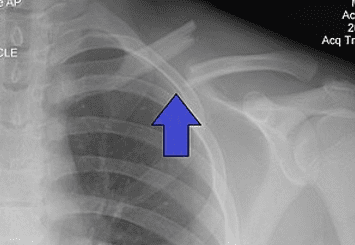
In most cases, initial X – rays are done to rule out broken bones.
Ultrasounds can be used to diagnose some ligament and tendon damage such as rotator cuff tears.
MRI is the best form of imaging but this does come at a higher cost and higher exposure to radiation. The MRI scan can identify bone, ligament and tendon injuries in the shoulder.
A CT scan is not usually performed in cases of the shoulder.
Instability:
If you have dislocated your shoulder in the past or continue to experience shoulder dislocations, you may have some instability of the shoulder. Normally you may develop a “dead arm”. You may also feel a sense of heaviness, numbness or an inability to move the arm which persists for a few minutes. If you are experiencing these episodes more frequently with less force, it is advised that you see your healthcare professional.
Treatment:
Non-surgical management involves a period of rest with a parallel shoulder strengthening program for stability. This is done when the injury is acute and non-recurrent.
Surgical management is opted for when there has been damage to the ligament and Labrum as well as ongoing recurrence of shoulder dislocation. Surgery is associated with a reduced rate of recurrence.

Rotator cuff:
The four muscles that make up the rotator cuff are Supraspinatus, Infraspinatus, Teres Minor and Subscapularis. Rotator cuff injuries are one of the most common disorders of the shoulder. It is believed that most of these injuries are caused by overuse of the shoulder. Often heavy lifting, sports involving the shoulder and repetitive shoulder movements are associated with rotator cuff pathology. These injuries cause pain and stiffness with overhead activity (eg: throwing a ball or putting a shirt on) and pain is worse at night. You may also feel some weakness in your injured arm because of pain.
Treatment:
A partial thickness tear in the rotator cuff can heal with non-surgical management. These are managed with physiotherapy exercises, corticosteroid (cortisone) injections and most importantly, time. It is important to know that the pain will improve over time.
A Full thickness tear in the rotator cuff will normally be managed with surgery. This is followed by immobilisation of the arm for up to 6 weeks in a sling. After these 6 weeks, you should begin a physiotherapy program in order to aid your recovery.

Acromioclavicular joint (ACJ):
This is a fairly common injury and normally occurs in athletes involved in contact sport or when falling directly onto the point of the shoulder. You may experience some pain and swelling in the upper shoulder. This pain can sometimes occur with no reason at all and it is important to voice this to your clinician.
Treatment:
You will be treated surgically or non-surgically according to the severity of your injury.
Non-surgical management includes a brief spell of rest and sling use for protection and healing. This is followed by early mobilisation of the shoulder and a subsequent strengthening program. Your physiotherapist can also assist you with taping in order to return to activity.
Surgical management is followed by a physiotherapy program as outlined by the shoulder surgeon. This is normally done for a quicker return to play in contact sports or when pain is severe and a trial non-surgical management has not worked.

Fractures:
These normally occur as a result of direct trauma to the arm such as a fall. They can be very painful and are usually associated with a lot of swelling around the area.
Treatment:
Depending on where and how severe the injury is, the doctor may opt for surgical or non-surgical management.
In either of these cases, you will undergo a period (6 weeks maximum) of immobilisation of the upper limb to allow for healing. At the end of this period, it is important to see your physiotherapist to begin rehabilitation of your arm.
Acute phase:
Immediately following an injury, you should be offered adequate pain relief. A sling can be very effective and can be combined with simple analgesia, anti-inflammatory medications and ice therapy.
Passive range-of-motion (ROM) exercises, including pendulum and active-assisted exercises, should be considered. You will be encouraged to maintain fitness (if comfortable) using a stationary bike or general walking.

Early Rehabilitation phase:
When your pain has settled and your ROM has improved to 60-70% of the unaffected side, you can progress with rehabilitation.
Exercises that might be useful in this phase include:
Late Rehabilitation phase:
You will progress to this phase when you have a normal (full and painless) ROM and 75% strength of the unaffected side.
The types of exercises that might be useful in this phase include:

Return to sport:
When you have a normal range of motion and more than 90% strength of the uninjured side, you can progress to return to sport. This should be done in a gradual manner.
A return-to-sport programme may involve:
Your shoulder injury will be treated and tailored to you. With most shoulder injuries, physiotherapy can be helpful in operative and non-operative management.
Early management or rehabilitation of your injury could go a long way in speeding up your recovery process and avoiding re-injury in the future.