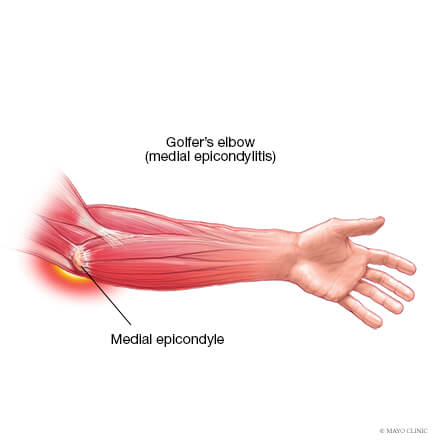
Medial elbow pain is also known as medial epicondylitis or golfer’s elbow. It is typically associated with pain on the inside (medial side) of your elbow and can spread into your forearm and wrist. This pain is the result of overloading and damage to the tendons that flex your wrist towards your palm.
Causes
This condition is triggered by damage to tendons and muscles which control your fingers and wrist. This damage is associated with excessive or repeated stresses- particularly repetitive and forceful finger and wrist movements, incorrect lifting, hitting and throwing techniques, lack of warmups and/or poor muscle conditioning.
Key risk factors for developing medial elbow pain may include smoking, obesity, being of in age bracket of 40 years old and over and undertaking repetitive activity with your arms for at least two hours daily. High risk occupations may include chefs, office desk workers, plumbers, construction workers, painters, butchers and assembly line workers. Those who partake in sports such as golf, racket sports, rowing, weight lifting and baseball are also at a higher risk.
Symptoms
Symptoms may be triggered suddenly due to a traumatic incident or may gradually develop over time and include but are not limited to:
Tenderness and pain is typically felt on the inner side of your elbow (particularly on the bony knob), and may refer along the inner side of your forearm and down to your wrist and fingers. It often worsens with certain movements. For example, bending your wrist towards your palm against resistance, or when squeezing a rubber ball.
You may feel stiffness in your elbow, and making a fist may hurt
You may experience weakness in your forearm, wrist and hand
You may experience tingling and numbness that can radiate into one or more fingers — typically to your ring and little fingers.
Diagnosis
This condition is typically diagnosed based on your medical and occupation history and a physical exam by your doctor or physiotherapist. To evaluate stiffness, strength and pain, your clinician may apply pressure to the impacted region and get you to move your elbow, wrist and fingers in various ways. You may also be referred on for imaging such as X-rays and Ultrasounds to aid diagnosis.
Management
A mix of non-surgical treatment options are effective for the majority of medial elbow pain cases, and self-resolves over time. You should rest your elbow and painful activities should be avoided. But it is very vital to maintain gentle movements of the forearm, elbow, and wrist through its range of motion.
Potential treatment options include:
Ice
Rest
Physiotherapy and acupuncture
Anti-inflammatory medications as recommended by your doctor or pharmacist
The use of a wrist and forearm brace or splint to support and rest your forearm
As your initial elbow pain lessens, your muscles around the elbow, forearm and wrist should be safely strengthened and stretched under guidance of a physiotherapist. Your physiotherapist will advise you on particular exercises, give you appropriate symptom management advice and take you through a personalised graduated rehabilitation program. If you continue to experience pain after 6-8 weeks of treatment, your physiotherapist can refer you back to your doctors, to consider administration of a cortisone injection into the elbow to help reduce pain and inflammation, and further referral onto see a specialist to seek guidance on other treatment options.
Prevention
Having a good comprehension of risk of injury and being conscious of your everyday activities may aid in the prevention of medial elbow pain. You should:
Adopt appropriate technique and form when undertaking repetitive activities or sporting motions
Keep up with adequate wrist, forearm, and shoulder muscle strength
Undertake gentle wrist and forearm stretches pre and post activities
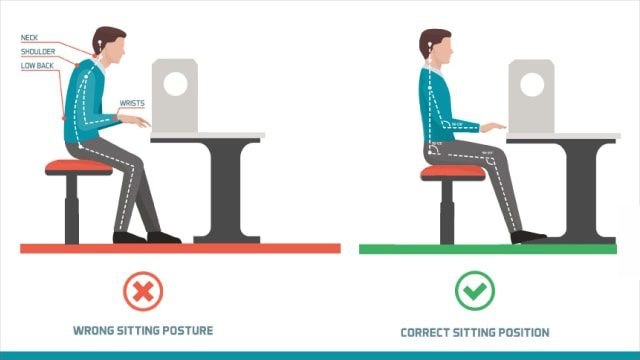
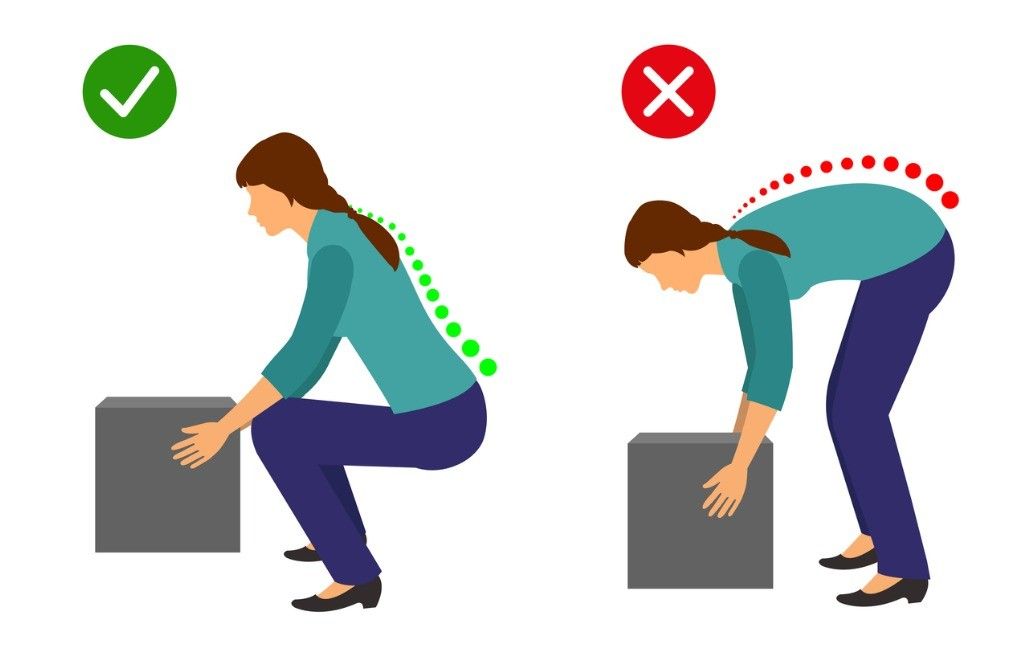
Adopt appropriate posture and body mechanics when lifting heavy objects to reduce joint strain- especially if doing so repetitively
Whether you are squatting racks of weights in the gym or squatting down to the floor to play with your children or simply squatting to sit in a chair – you are still squatting.
Truth of the matter is, squatting is more than just an exercise. If you think about it, it is a functional movement we all do many times in the day.
Knee pain from squatting is a common compliant. Although it is common, it doesn’t mean it is normal.
More often than not, the problem doesn’t only lie at the knee joint. We have to understand the complexity of our body in how our knees are directly linked with how your hips and ankles are moving. So, the purpose of this blog is not only to help you understand the basic mechanics involved in the legs when you squat, but also to help you perfect your lifting craft in the gym.
A bit on what is a squat?
Squatting is characterized as a ‘compound movement’ – fancy fitness lingo that simply means, multiple joints and muscles are moving and working in harmony to contribute to the very movement of squatting.
So here is a checklist to help you find the missing links.
Squatting check list
1. Foot arches
Feet are the foundation to our body. From a balance perspective we can go as far to say that steady the feet, steady the rest of the body. So, what happens at our feet is extremely important to consider when we talking about knee pain in general, let alone, knee pain when squatting.
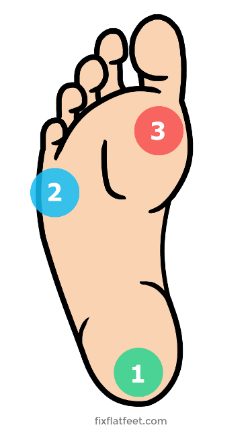
Foot stability can be best explained using the analogy of a ‘tripod’. As tripod has 3 points of contact with the ground, so should our feet ideally.
The three points of a contact, as in a tripod looks like this in our feet.
Ball of the big toe
Ball of the 5th toe
Heel
Keeping this in mind, lets assess the foundation of your body – Your feet with this small exercise.
Take your shoes and socks off. Stand up tall, plant both your feet flat on the ground. Take a look at both sides individually. What do you see?
Either of your feet collapse in?
Are either of your arches diminished?
Take note of it. Next, remain standing and focus on what you feel at sole of your feet.
Think about the 3 points of contact – the tripod.
Do you feel you have evenly distributed pressure?
Take note.
Now stand on one leg – think about the same TWO things the arch and the pressures.
Which way did your foot go?
Which points of contact in the foot had more pressure?
Did your toes 3-5th lose contact from ground?
If your foot caved in and the last 3-5th toes lost ground contact, then your foot pressure is likely to sit between big toe, the base of 2-3rd toes and heel, suggesting you have a narrowed base of support. This will force the knee, hip and the rest of your body to follow in the direction, creating risk of building up unwanted pressures in others areas of your body. Before you know it, unwanted pressure results in inflammation and pain.
It is important that you consider this of high value and practice on pressure control and arch control before your look at the overall picture of squatting.
2. Ankle mobility
Your foot and ankle are closely linked – between them there are 28 bones, many muscles, ligaments and connective tissue. These anatomical structures work together to provide stability and mobility of the joints – considered KEY essentials to squatting.
Too much or too little flexibility in the ankle can be a problem. In most cases, ankle injuries result in stiffness, a hinderance to simple functional movements.
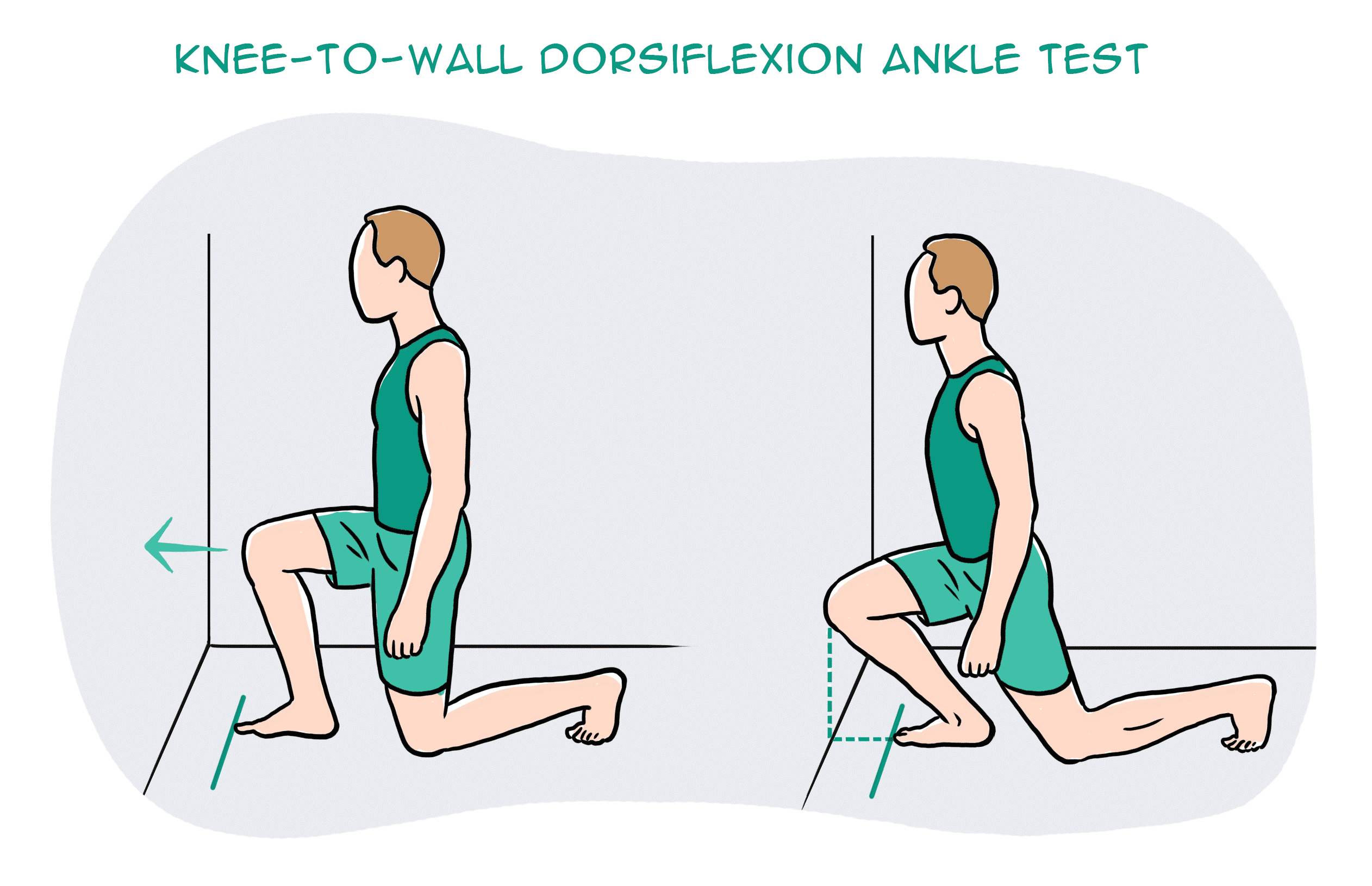
So, let’s take a closer look at your ankle with a simple mobility test.
Kneel down in front of a wall. Signal a thumbs up and measure the width of it from the wall and mark it. Place your foot on the line and drive your knee forward to the wall. Make sure you drive your knee straight forward without caving in or twisting in with your hips.
What do you see?
Can you touch your knee to the wall?
What about the other side?
Consider what you feel.
One side feels almost effortless, the other side doesn’t?
It is not uncommon to notice that the unaffected side may not be as flexible as you thought.
This is point to note – you have just discovered a link and a potential cause of your knee pain.
You need focus on stretching the muscles of your leg in a way that similar to ‘squatting’ – here is a good one!
Box ankle stretch
Use a box or a chair, plant your foot flat and rock forwards until you feel a stretch in the calf and ankle. Remember to make sure your knee doesn’t cave in or your body doesn’t twist. Do this for 20-25 repetitions, 2-3 sets. Re-test yourself.
3. Hips
Your feet are directly tied to your hips. So, the action of your hip and feet should be working together for good purposeful movement.
Here is a quick way to check this yourself:
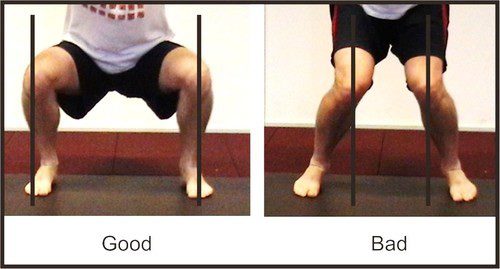
Stand tall, with your feet planted shoulder width apart. Drive your knees out to the side. You will notice your foot arch lifts.
It might be a very small amount, but worth taking note. Because, this is no different when you are squatting. If your knees collapse in, it may mean that you are not recruiting the key muscles of your hips that prevent the knees collapsing.
So, driving your knees out to match the alignment of your hip-ankle not only lifts the arches but begins the process of recruitment patterns of hip muscles to engage.
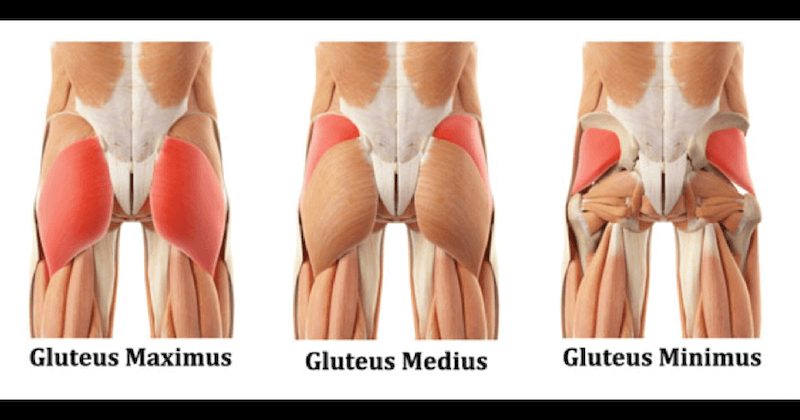
The common deficit contributing to your knee pain may be weak gluteal muscles.
Gluteal muscles are powerful muscles of the lower limb. They are a group of three muscles, each with slight different function
Gluteal maximus – hip external rotation, hip extension
Gluteal medius – hip abduction, internal and external rotation, extension
Gluteal minimus – hip abduction and internal rotation
Banded squat
Banded squats are a great way to activate your gluteus. The band not only provide resistance but provides sensory information to help you learn to push into it, therefore avoid knees from collapsing in.
If you have a lighter level resistance band, place this at knee height.
Descend in to a squat position with emphasis on pushing you knee out into the resistance band, until you reach the hip-knee-ankle alignment.
Do this 15 times, 3 sets.
For starters, work at a level that is easy for you.
Build the reps ups as you gain confidence
Weak or inadequately recruited muscles could be a result of stiffness hips.
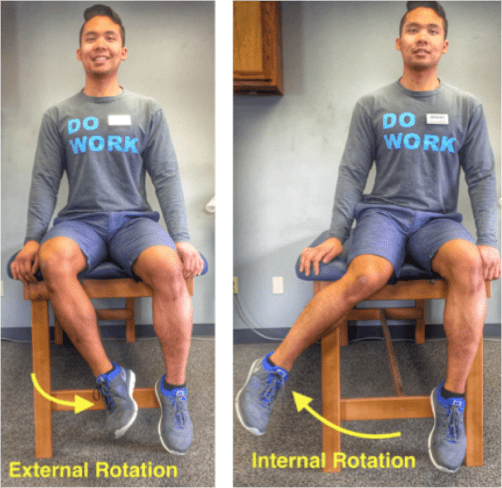
To check your flexibility, try this next test:
Sit on tall on a chair. Feet planted flat on ground at shoulder width apart. Test one leg at a time. Keeping your thigh in contact with the chair, drive your knee out to the side (internal rotation). Now try going inwards (external rotation).
What do you see?
Can internally rotate higher? External rotation is difficult? Or vice versa?
What do you feel?
Takes more effort going one way than the other?
Unlock the hips with this beginner hip stretch.
Sit upright on a chair. Cross one leg over on the other. You should feel a stretch in the buttock region. If not, progress by leaning forward with an upright posture. Hold for 15-20 seconds. Repeat 3-5 times.
Perfecting your squat
Perfect practice makes perfect. Now bearing the rules of movement in mind, practice your squats.
Some tips to help you better practice:
Do not worry about the depth of your squat
It’s the quality not the quantity. So as you begin to learn and adapt these principles, only squat down to a level where you feel in control of your foot, ankle, knee and hip.
Use a mirror
Visual learning is a great tool! It provides for a greater ability to correct your mistakes and perfect that ‘quality over quantity’ rule.
Start with barefoot
This allows you to connect the sensory receptors in the soles of your feet to the ground, making it much easier to learn the tripod grip.
Still having pain?
Remember, the complexity of our body and the complexity in how we move as whole can be the result of your knee pain. So, if you are still having pain – its time you get it checked.
There can be multiple reasons why your knees sound like popping popcorns or grating stones when you squat.
Generally popping in the knees is attributed to stiffness of the quadriceps muscle and the fascia that surrounds the knee joint. Overtime, stiffness causes pressure to build up under knee cap, which on movement can cause a sudden release causing a ‘popping’ sound. As worrying as it may be, most of the time popping noises in the knee without pain is NORMAL. However, for others the noise can be accompanied with a grinding sensation under the knee cap which is painful. This suggests there is an underlying pathology that needs to be addressed.
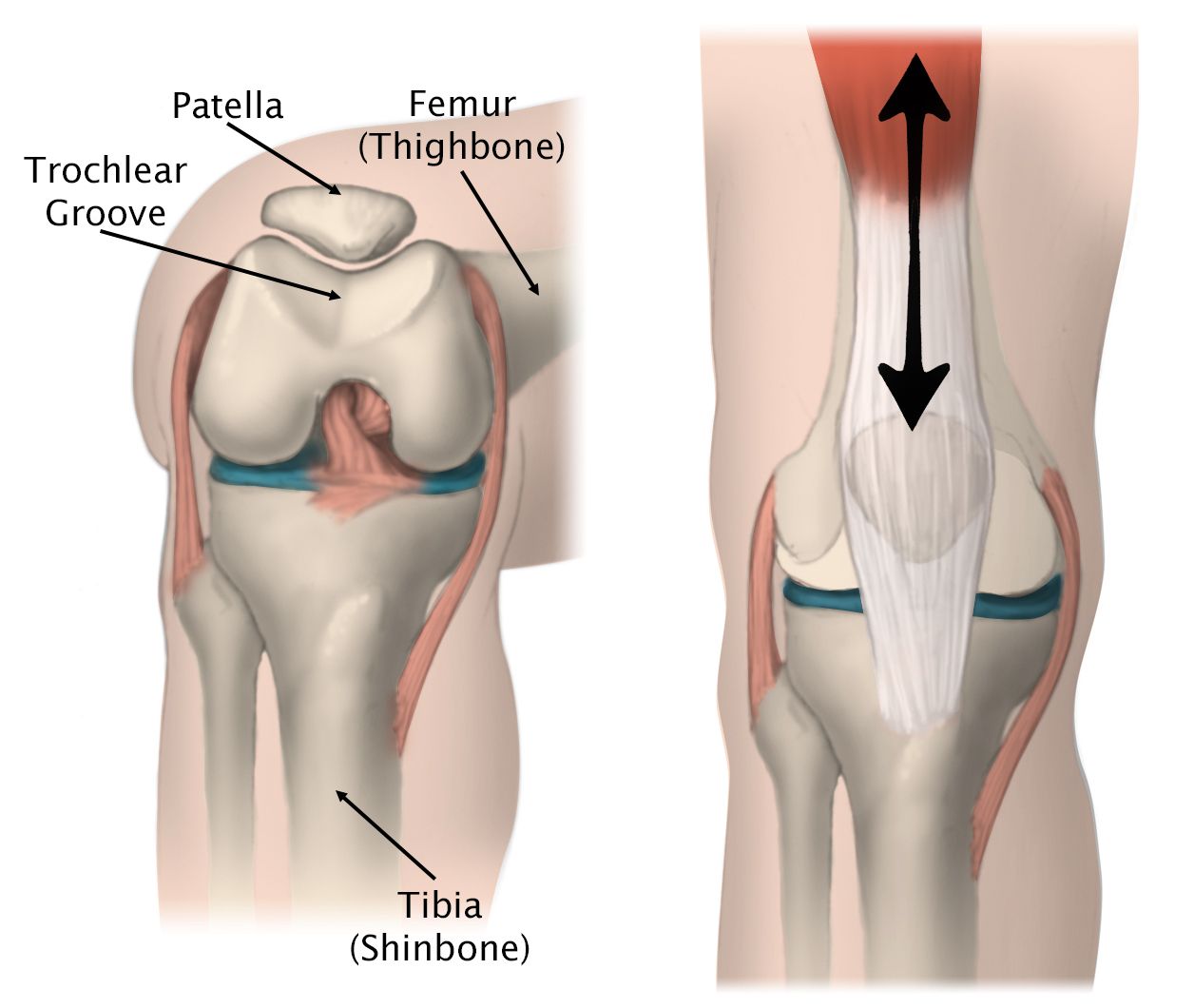
This is something we would clinically consider to be Patella Femoral Pain Syndrome aka Runner’s knee – an umbrella term that encompasses the idea of dysfunctional knee cap tracking.
When you straighten and bend your knee, naturally your knee cap tracks up and down between its groove (trochlea groove) – like a train moving up and down a train track.
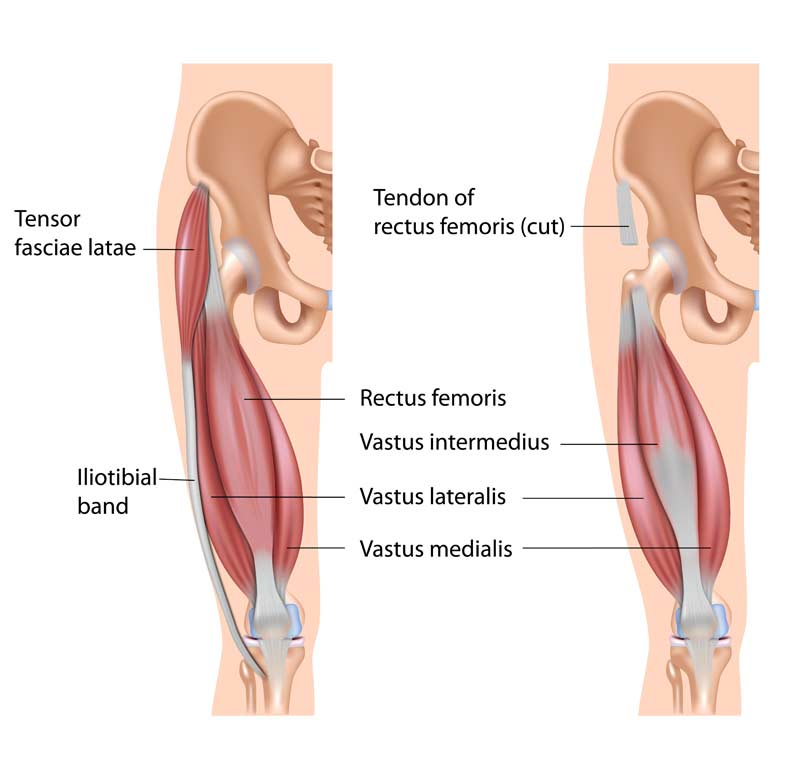
When the quadricep muscles on the outside (vastus lateralis) and inside (vastus medialis oblique) part of the leg are working in synchronization as they should, your knee cap is able to track up and down properly. However, if the quadriceps muscle (Vastus lateralis) is overly activated and the fascia (Iliotibial band & lateral retinaculum) on the outer part of you knee cap is excessively stiff, the knee cap gets pulled to the outside.
Essentially the train is being pulled and tilted more to the outside. Eventually overtime, repetitive or violent lateral pull of the knee cap increases friction in the knee grating the smooth underside of the knee cap called, chondromalacia. Additionally, the constant pulling and stiffness of the lateral side will cause stretching on the inside of muscles. On top of that, pain and swelling will cause the muscles in the inside of the leg to shut down.
Here are two steps to managing your symptoms.
STEP ONE
Foam roller or tennis ball
Instructions:
Lie on your front and place the foam roller underneath your leg.
Bend the opposite leg and bring it out to the side to help you move back and forth.
Roll the entire length of the thigh muscle, staying off the knee joint.
Make sure you move through the length of the muscle close to the knee cap as you can. You should be looking for stiff spots in the muscles and any sore spots you feel concentrate on it for couple of seconds and work deeper in to the tissue. You should also move in the inside and outside of the quadriceps muscles. Do this with you knee straight and then move into knee flexed position to optimize the release.
For a more concentrated release, use a tennis ball or a lacrosse ball especially at the quadriceps tendon where much of the stiffness is likely present. The reduced surface area of the ball allows you to work on specific spots a lot better to break down deeper areas of stiffness and create more mobility.
Do this mobility routine for 1-2 minutes
Quadricep stretches
Start in a standing position. Use support if required for balance.
Raise one leg behind you grabbing hold of your ankle, or your lower leg.
Lift and hold for 20-30 second, and then repeat for the other leg.
Get into a lunge position with back leg flat on floor
Bend your knee and slowly pull your leg into a stretch
Hold this stretch for 20-30 seconds
For comfort place a rolled face towel under the knee cap
Modified quadricep stretch
For some people if kneeling down is irritating for the knee you can modify the stretch.
Rest your leg on the chair with your foot against the back rest
Make sure your stance leg is far enough in front of the chair
Lunge forward until stretch is felt
Do this for 20-30 seconds.
NOTE: Long duration stretches of over a minute and more can decrease the potential for you to create strength and power in those muscles during your workout. So, prior to your workout focus on short duration stretches.
Functional mobility stretch
Deep squat sits are great to expand the stretch. If your symptoms are not aggravated, try deep squat sits for 30 seconds up to a minute.
Stand with feet shoulder width apart
Point your feet out to about 45 degrees
Sit in to a deep squat keeping the pressure evenly distributed across feet
STEP TWO
Now that you’ve resolved the stiffness in the lateral portion of your knee, next step is to address the muscles imbalances caused by pain and swelling. That is, turning back the firing of the quadriceps muscles.
An effective way to address this, is by doing what we call close chain exercises – these are exercises done where your feet are on the ground, such as squats. Initially you want start slow and high. Mini squats are great because they allow you to strengthen your quadriceps without putting too much compressive forces into your knee. As you get comfortable, advance to a deeper squat and slowly begin to work towards building you strength by adding on weight.
Mini bodyweight squats
Stand behind a chair or table and place your hands onto the back rest.
Keeping your back straight, bend both knees into a semi-squatting position, allowing your hands to slide forwards.
Your hips should travel backwards as you counterbalance by leaning your chest forwards.
Push through your buttock and thigh muscles as you return to standing, and repeat.
Deep bodyweight squats
Hold on to the dumbbell, keeping it close to your chest.
Step your feet wide apart and turn the toes out slightly.
Drop down into a deep squat position, keeping your feet on the floor.
Control the movement back to the start position.
Caution: Avoid deep squats especially if you have ongoing grinding pain. Do not push in to pain, as this will only increase the forces and worsen your symptoms. At this point, it is highly recommended that you come in to see a physiotherapist to examine a potential underlying pathology.
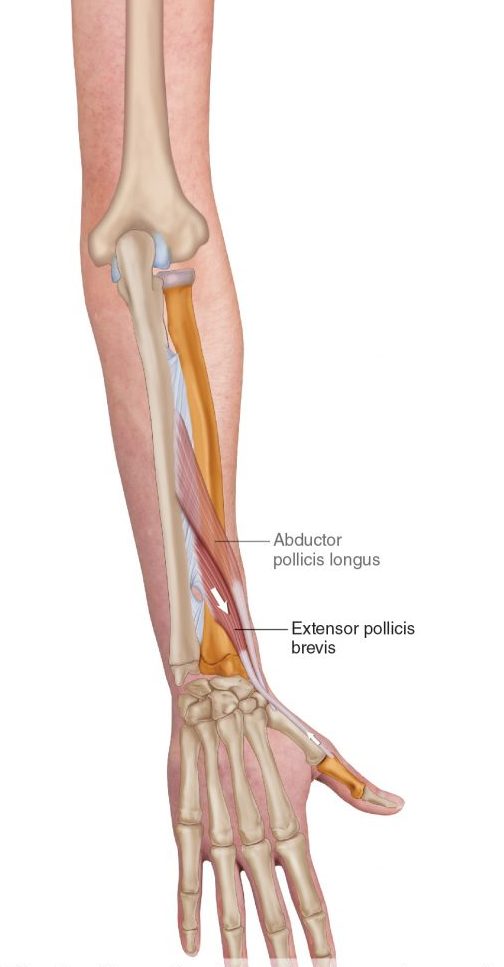
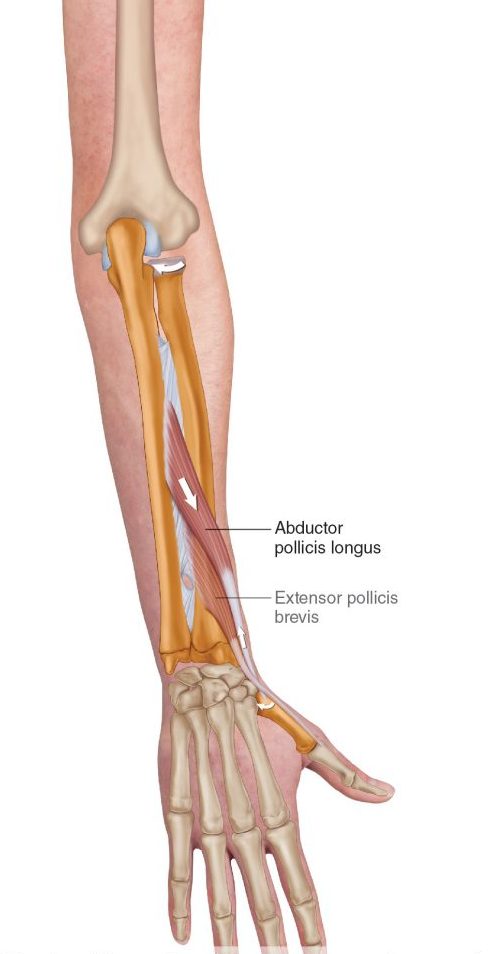
De Quervains tenosynovitis is a painful condition caused by inflammation of two prominent tendons that are located at the wrist and thumb.
The two tendons called the Extensor pollicus brevis and Abductor pollicus longus originate from the middle of the forearm travel down towards and over the wrist to insert into the thumb. Collectively they function to extend the thumb, whilst abductor pollicus longus extends and also abducts the thumb (lifting thumb up to the ceiling).
What causes it?
The most common cause of De Quervains tenosynovitis is the repetitive overuse of thumb and wrist whether it is occupational or hobby related. For example, the repetitive thumb movement whilst using scissors by hair dressers, landscapers using shears or whilst gardening). Trauma to the tendons from injuries to the wrist or the thumb can cause inflammation of the tendons.
In some cases, age related degeneration of the tendon sheath or underlying conditions such as rheumatoid arthritis increases the risk of the developing De Quervains tenosynovitis. Hormonal changes resulting in fluid build up in young mothers can commonly result in De Quervains tenosynovitis.
Symptoms
Commonly your symptoms may include:
Pain located at base of your thumb
Pain elicited by movement of thumb (gripping or making a fist)
Grating or snapping feeling
Tightness in the wrist
Swelling surrounding the base of thumb and wrist
How is De Quervains tenosynovitis diagnosed?
Your doctor or physiotherapist will be able to diagnose the condition based on your symptoms and after doing a thorough movement assessment to rule out any other potential diagnosis.
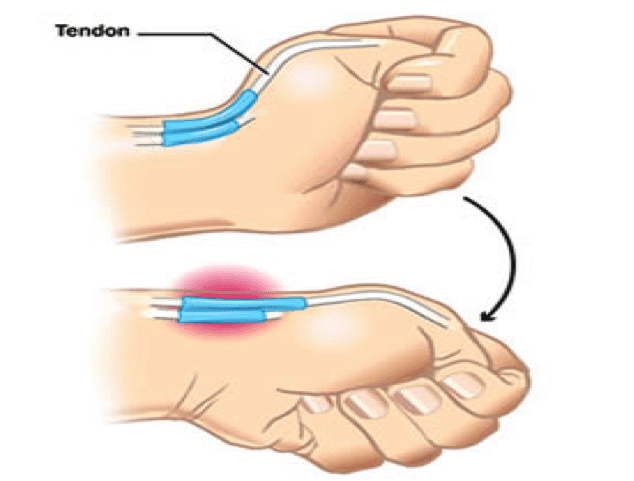
Finkelstein test is used to elicit symptoms to confirm De Quervains tenosynovitis.
How to test:
Wrap your thumb with your fingers.
Slowly bend your wrist down
A positive test would elicit pain at the site of the two tendons.
Radiological investigations in lights of ultrasound and an x-ray might be recommended for further investigations, particularly to confirm clinical diagnosis or to rule out any other possible causes of De Quervains such as osteoarthritis.
What treatment options are available?
Conservative (non-surgical) management
Conservative management measures are generally recommended as the first line of management for mild to moderate symptoms. This is because up to 60-70% of symptoms are likely to improve over a period of 6-8 weeks of regular physiotherapy intervention. In this period, the following strategies are recommended by your therapist to fast-track your recovery
Rest and application of heat or cold packs
Avoid repetitive use of thumb
Pain medications (anti-inflammatory medications) such as diclofenac or ibuprofen
Splints or braces
Steroid injection
Surgical management
In more severe cases when conservative management has failed, surgery may be recommended by an orthopaedic specialist or surgeon.
Prior to your surgery you will have the opportunity to thoroughly discuss with your surgeon the details of the surgical procedure and about the post operative rehabilitation process.
Surgical procedure
Surgery may be performed under general or local anaesthesia. A small incision is made at the wrist and thumb region. The covering of the tendons (sheath) is then separated and expanded to provide the tendon space to allow the tendon to move smoothly within the sheath. After this the, the incision in then sutured with a firm dressing applied over the suture site.
While you recover from the surgery, an information sheet with post operative guidelines will be provided to you by your surgical team. It is important that you must follow the guidelines recommended by your surgeon for optimal recovery.
In most cases your will have a follow up with your surgeon few weeks after your surgery to check your wound healing and your progress. You are often times referred to physiotherapy for strength and conditioning of your wrist and hand movements to facilitate your recovery.
Deadlifting is one of the most very versatile exercises in the gym. There are about 11 variations of the exercise, whether you are doing it with dumbbells, kettle bells, barbells or traps bars. The variations and the technical complexity of the exercise can be extremely intimidating for some, especially for those who are combating lower back pain.
While there are multiple factors to consider when determining that causes of lower back pain, the technique and the execution of the exercise is by far the most common cause. Therefore, this blog will focus on the common mistakes you are likely making in the weights room resulting in your persisting lower back pain.
What are the benefits of deadlifts?
Deadlifting is one of the most respected exercises in the gym, often referred to the king or queen of all compound exercises. This means that at one shot of movement you are activating almost every key muscle in your body. Including your heart – Yes, the heart!
Before we elaborate of the musculoskeletal system, here a little interesting information on why the heart. For starters, the heart is a muscle. Its prime function is to supply nutrients and oxygenated blood throughout the body for effective organ functioning. To do so effectively it regulates the blood pressure and heart rate. So yes – to simply put it deadlifts when done correctly as advised by a health practitioner can have tremendous health benefits on reducing heart rate, blood pressure and improves overall conditioning of the cardiovascular system.
As sides that, from a musculoskeletal stand point there are strategic strength, power, and coordination and aesthetic that are achieved. In the era of computers and laptops and sedentary jobs – Working at a desk for 7-8 hours a day, we become more dominant in using the muscles in the front of our body (the anterior chain) and the muscles in the back (posterior chain) tend to be inactive and weak.
For this reason, the deadlift is particularly regarded as the single most beneficial exercise one can do that targets the entire body at one go, perhaps with more emphasis on the posterior chain.
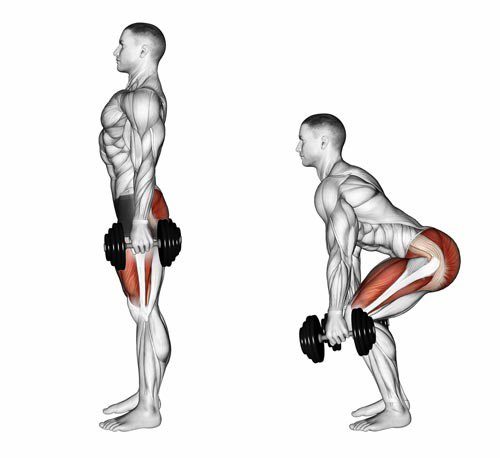
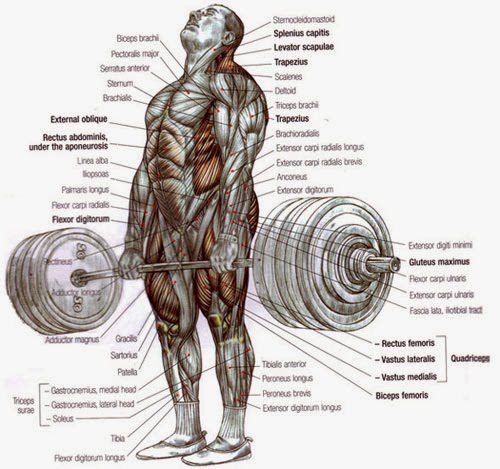
What muscles are used?
As seen in this picture on a ‘conventional variation’ of a deadlift almost every muscle is highlighted – from the gripping the bar with the hands to gripping the ground with the feet.
core muscles
gluteus
hamstrings
adductors
quadriceps
Technique faults to consider
1. Poor core stabilization
Core-stabilisation is the foundation fundamental to almost any given exercises in the gym, let alone a deadlift. When you are told to ‘brace’ your core – it’s not the sucking in of your belly or holding your breath. It about activating or ‘tightening’ up the key of your ‘core’ to contain the pressure (intra-abdominal pressure) from within. This is absolutely crucial in creating stability and preventing overloading for your spine, especially when lifting heavy.
For the simplicity of this blog, information around intra-abdominal pressure is kept brief and explained using the ‘soda can’ analogy.
What exactly is ‘core’?
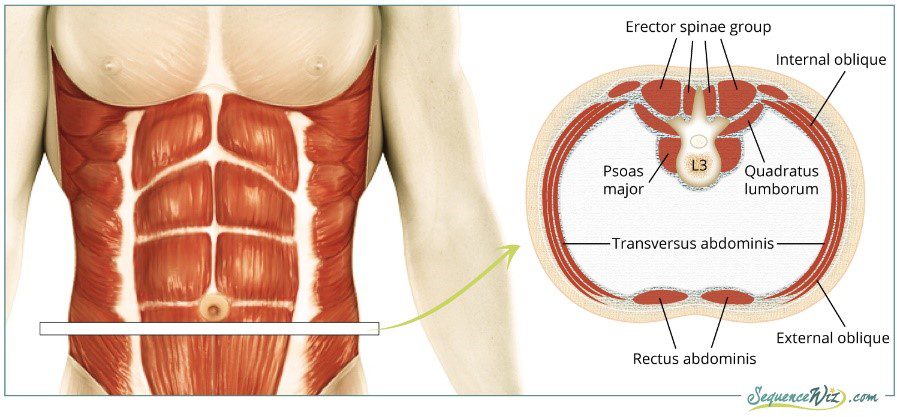
What many people don’t know is that core is more than just abdominal muscles. The core aka the corset of our mid-section includes the deeper and the outer muscles.
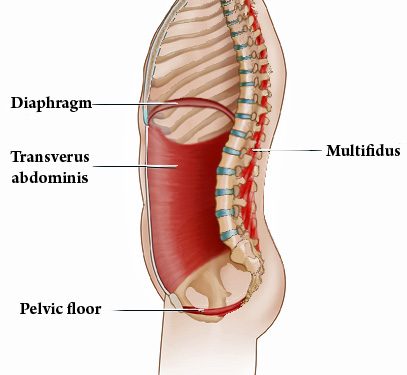
DEEP CORE
The deeper core, regarded as the main ‘core subsystem’ as seen in this picture essentially involves four muscles strategically designed for maintaining pressure (intra-abdominal pressure) in our mid-section.
OUTER CORE
The outer core muscles as shown are stronger and bigger muscles covering most of the surface area of our mid-section. When activated, they support the the deeper core muscles in maintaining the intra-abdominal pressure. They include:
Erector spinae
External oblique
Rectus abdominis
Latissimus dorsi
How to brace your ‘core’
Sit or stand tall with your hands resting against your abdomen.
Take a deep breath in as though you are storing the air in the base of your lungs. As you do this must feel your abdomen ballooning out.
Now, tighten your abdominal muscles firmly, as would before you cough.
Then gradually released your breath whilst keeping your abdominals tight. As you do this you will feel pressure building inside your abdomen.
Repeat this cycle until you get comfortable with the bracing.
2. Incorrect set up, initiation, lift and descend
INCORRECT SET UP
Most people approach the barbell with a squat stance. This means the hips drop too low in line with the knees and the bar is too far. This causes you to stretch your arms forward to reach the bar which prevents the optimal latissimus recruitment needed to secure the bar for the lift.
Tips:
1. Approach the barbell and stand with your feet shoulder width apart.
2. The barbell should be directly in line with your midfoot.
3. Feet can be pointing straight or slightly off centre positioned out.
4. Your knees should be tracking in the same direction as your feet.
5. Bend down to reach the bar and position your hands just outside your knees using an overhand grip. The bar should be close to your shins.
6. From a side view: your hips should be positioned between your shoulder blades and your knees.
7. The barbell should be directly underneath your arm pits.
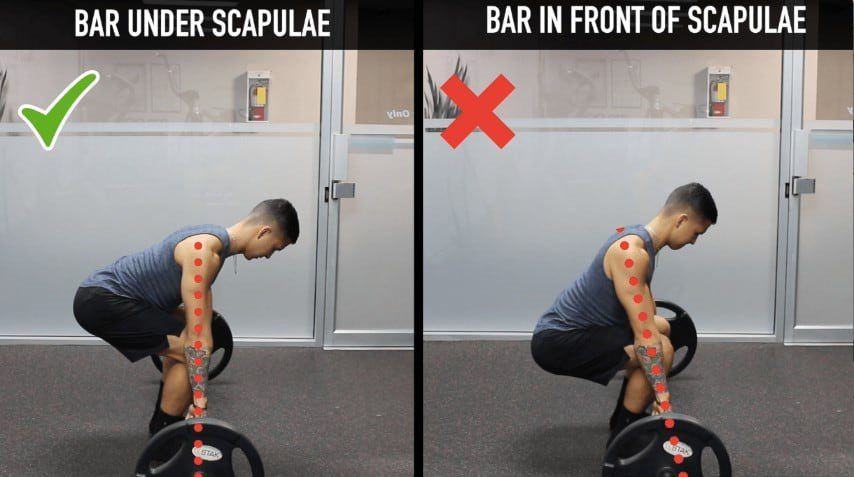
INCORRECT INITIATION
Head up and chest up, hyperextended back or head up, chest collapsed and rounded back are the two most common lifting mistakes seen when deadlifting. This means there is inefficient requirement of larger muscle groups in the lower extremities to be the ‘main drivers’ of the lift, instead heavy amounts of load is places on the spine and its surrounding soft-tissues (ligaments, muscles, fascia). Therefore, the risk of lower back injury is significantly greater and depending on the weights used and the training intensity, injuries can range from simple overly fatigued muscles to significant soft-tissue strain or in worst cases a herniated disc injury.
Tips:
8. From side view: align your torso with shoulders and hip
9. Activate the latissimus by squeeze your armpits down and slightly pinching your shoulders blades back
10. Before you lift, think about the lift. Rather than pulling the weight up with your upper body, think of bracing or stiffening your upper body and then pushing the ground away from your body with your feet and straightening your knees and your hips (similar to how you push the weight plate away during a leg press)
THE LIFT & DESCEND
Tips:
11. With your posture now set and body braced, push the ground away with your feet to straighten your knees and hips to stand up tall. From the time you initiate the lift until the barbell touches down to the ground, it should travel in a vertical line.
12. When standing tall, avoid hyperextending with your back. Make sure your body remains in the braced position ready to lower the bar down.
13. Push your bottom back, this will allow you to realign your arm pits with the barbell to steady your decline and allow the barbell to travel in a vertical line to the floor.
To consider:
While these are a few key principles to consider before you execute a perfect ‘conventional deadlift’, there is really no ONE size fits all . Technique to setting up and lifting should be strictly individualized based on your height, flexibility, lifting experience and goals.
So before you consider this all intimidating exercise, whether you are a novice, or someone who is getting back to action after an injury, follow these simple steps:
Start slow and start low on weights.
Have a gym partner spotting you, an extra pair of eyes to watch your technique will always help
Or simply use a mirror – and practice, practice and practice.
It all comes down to efficiency, using the correct muscles to their best activation range as much as possible. So that when you reach close to the fatigue point it’s the major muscles such as the glutes, hamstrings fatiguing not the smaller less robust lower back muscles.
“My neck feels so tight and knotted up”, “can you give my shoulder a rub, there are so many knots in them”, etc.
We have heard people referring to these terms time to time in our daily life, but we have hardly ever put real interest in finding out what the real meaning behind it. So, what are muscle knots? What causes them? But most importantly, what can we do to treat and get rid of them?
What are muscle knots?
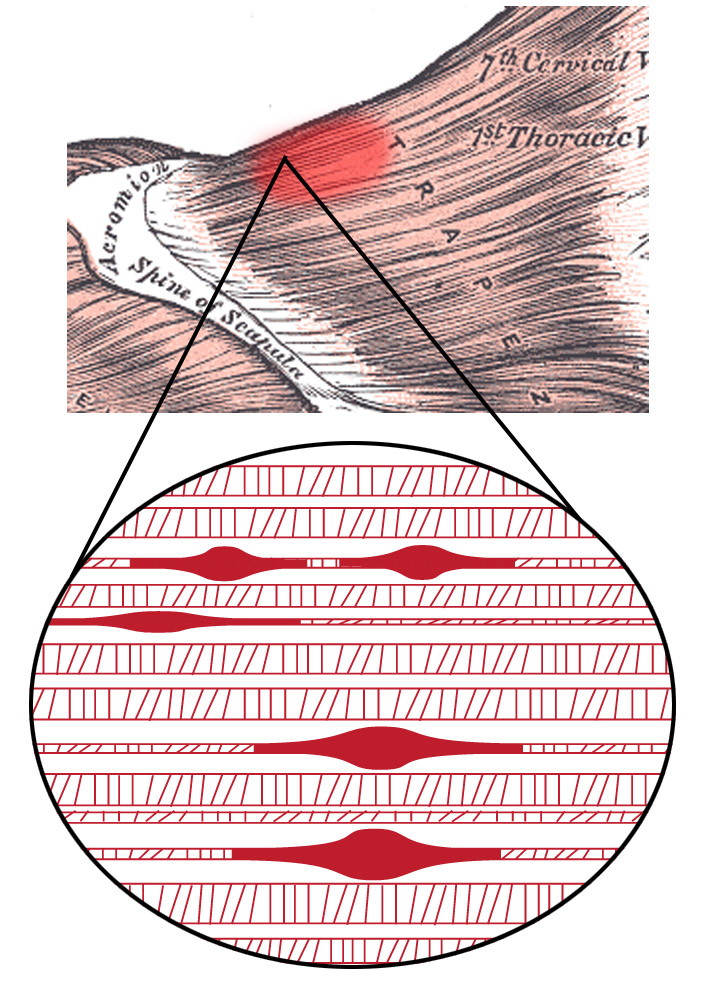
Muscle knots are jargon term for a more scientific term of trigger points. A trigger point is a hyperirritable spot and a hard, palpable nodule in a taut band of the skeletal muscle that can be either extremely painful with external pressure or compression onto it such as palpation (they are usually called active trigger points), or not very painful at all even with palpation (these are usually called latent trigger points). Myofascial trigger points can lead to pain, weakness, muscle dysfunction, and sometimes loss of range of motion secondary to muscle tightness.
Often these trigger points can lead to a common condition known as myofascial pain syndrome. It can be an acute condition resulted from a certain overuse injury/event, or chronic condition which resulted from years of repetitive work. It does not only involve the primary muscle, but also its surrounding connective tissue known as fascia (fascia is a thin connective tissue casing and holding all the soft tissues together – imagine that when we process a piece of meat, there is a thin white film on top of the meat that we normally try to remove). Trigger points also cause the muscle to be more sensitive to pain with sensitization of the nerve tissue.
Fig 1. Multiple trigger points in the trapezius under cellular view
Most common types of myofascial trigger points:
Primary or central trigger points are those that cause severe pain locally at the pressure with irradiation according to referred pain map. Usually are based around the centre of a muscle belly – and it is almost always the active trigger points.
Secondary or satellite trigger points arise in response to existing central trigger points in surrounding muscles. They usually spontaneously withdraw when the central trigger point is healed. Can be present in the form of a cluster – and most of the satellite trigger points are latent ones, but they can eventually become active if it is provoked/aggravated.
Etiology/causes of myofascial trigger points:
Muscle knots or trigger points are formed from various reasons, but most common causes are overuse or trauma. However, our bodies are very complex and they can also be formed due to psychological stressors. Muscle knots or trigger points can also be formed from enough stress in the soft tissues with sustained abnormal/bad postures or repetitive activities, and they can begin to elicit pain.
Causes of trigger points:
Aging
Injury sustained by a fall, stress, or birth trauma
Lack of exercise – commonly in sedentary persons between 27.5-55 years, of which 45% of men
Bad posture – swayback posture, telephone posture, cross-legged sitting
Muscle overuse and respective microtrauma – weightlifting
Vitamin deficiencies – vitamin C, D, B; folic acid; and iron
Sleep disturbance
Joint problems and hypermobility
Myofascial trigger point referred pain:
Active trigger points and muscle knots do not only respond to pressure or palpation. They can also be inducing muscle stiffness that spreads its painful ache out and around a central myofascial trigger point. When this happens, these muscle knots can spread and refer/radiate pain towards all corresponding areas. In 1983, two experts in myofascial pain syndrome and its referred pain, Janet G. Travell and David G. Simons, have carried out a thorough research and produced a map of referred pain pattern for various common myofascial trigger points and they called it “Myofascial pain and Dysfunction – The Trigger Point Manual”. Today, specialist clinicians such as chiropractor, osteopath or physiotherapist like us still refer to the textbook in our practice time to time.
Fig 1. Example of infraspinatus’ myofascial trigger point referred pain
Signs and symptoms of trigger points or muscle knots:
General sore spots, sensitive to pressure, primarily in muscles.
Affected limbs may feel a little heavy, stiff and feeble.
Pain mainly elicits at a localised spot that you can almost pinpoint it.
Pain can be dull, aching, and nagging.
There is usually no clear mechanism of injury, but flare-ups can be exacerbated in response to extremes of position, or exercise.
Pain is usually in episodes but episodes can last a long time (for days, weeks, or months).
The pain may move around and even to the opposite side of the body. However, it is still a very uncommon symptom, but a distinctive one of trigger points.
Any heat modalities such as hot showers, baths and heat packs provide pain relief.
The pain is not strongly linked to movement as a low back pain or ankle sprain would be.
What can physiotherapy help to treat myofascial trigger points?
Physiotherapist is well-trained to treat the condition with a variety of useful tools and techniques in together with their knowledge to approach the condition most effectively.
Trigger point massage involves applying sustained pressure directly over the irritable trigger point to create a hypoxic environment for the knot, which reduces blood and oxygen supply. The main goal is to relax and free up the contracted/knotted muscle fibers at the trigger point to produce a gradual relaxation.
Dry needling therapy is a treatment modality where your trained physiotherapist inserts a few fine needles aiming at the trigger points of the concerned muscle. This causes a cascade of chemicals to be released from the muscles, which can cause a local twitch response, which is a contraction and RELAXATION of the muscle fibres in the contracted tissue.
Massage, especially deep tissue massage.
Passive stretching exercises.
Postural advice/education that can be contributing to the eliciting of trigger points.
Education regarding self-release methods you may apply at home to help relieving pain, muscle knots and myofascial trigger points, such as foam-rolling, massage balls, etc.
RSI is typically defined as an overuse disorder- a gradual build-up of overload to nerves, tendons, and muscles arising from repetitive movements or activities. Repetitive use of the same motions leads to inflammation and damage to these soft tissues. This disorder mostly affects the upper limb- particularly the elbows, hands and wrists.
Causes
Possible causes of RSI include but are not limited to:
Undertaking the same and repetitive movements and stressing the same muscle groups
Working in cold environments
Assuming a sustained and/or awkward posture for prolonged periods of time
Undertaking a particular activity for prolonged periods of time with no rest-breaks
Frequent and prolonged use of vibrating equipment
Adopting poor postures from working at inappropriately designed workstations
Undertaking a motion which involves carrying and/or lifting heavy items
Symptoms
RSI leads to a gradual development of a broad variety of symptoms, which range from mild to severe in severity. RSI particularly affects the muscles and joints of your wrists, hands, elbows, forearms, shoulders, neck. Having said this, RSI can affect other areas of the body as well.
Common symptoms may include:
Pain
Tingling
Cramping
Increased sensitivity to heat and cold
Tenderness
Fatigue
Loss of strength
Throbbing
Soreness
Achiness
Stiffness
Struggling with typical activities of daily living, such as gripping and twisting motions, carrying light weights, writing, kitchen prepping, dressing, personal cares etc
You may develop these symptoms when you undertake a task repetitively for a period of time, and can settle when you stop. Symptoms may settle over a few hours or over the course of a few days. However, if left untreated or is poorly managed, a minor RSI may gradually progress to a nasty chronic injury.
Diagnosis
If you experience mild discomfort whilst completing particular activities at home or at your job, it is a good idea to see your GP or physiotherapist to talk about RSI. But an RSI is not always simple to diagnose as there is no particular clinical test for it. Your GP will enquire about your medical history, occupation and work environment, and other activities to attempt to identify any repetitive motions you undertake that may be the cause of your symptoms. A physical examination will be undertaken, where they will assess your movement, check for pain, inflammation, sensation, tenderness, strength and reflexes in the impacted body part. RSI may be triggered by specific health disorders like bursitis, carpal tunnel, tigger finger, ganglion cyst, or tendonitis (inflammation in your tendons). Your GP can refer you on further diagnostic tests such as X-rays, Ultrasounds, blood tests, MRIs, nerve conduction tests etc, to determine if these underlying disorders may be the cause of your symptoms. You may be also be referred onto a physiotherapist and acupuncturist for conservative treatment and management for mild-moderate issues. If symptoms persist, you will then be referred onto a specialist.
Management
Initial treatment options for the management of RSI symptoms is conservative. This includes:
Rest, Ice, Compression, and Elevation (RICE principles)
Taking regular breaks between tasks and looking after your posture
Undertaking your activities and movements with appropriate form and posture
Intake of Nonsteroidal anti-inflammatory drugs (NSAIDs), both oral and topical as prescribed by the GP
Use of cold and heat to the impacted area
Administration of steroid injections into inflamed joints and tendons
Tailored exercise prescription from physiotherapists to correct posture and strengthen and stretch affected muscles
Acupuncture
Stress reduction and relaxation training
Use of splints and braces to help protect and rest the affected muscles and tendons
Ergonomically appropriate adjustments to your workstation and work environment may be recommended by your physio and GP- for example resetting your desk and chair if you’re working at computer, and alterations to your equipment and activities/motions to lessen the strain and stress on your muscles and joints. Surgery may be necessary in some cases.
Prevention
Minimizing repetitive actions particularly if they involve the use of heavy machinery or vibration. Improving your working posture and work-environment as well a taking regular breaks. Employers often undertake risk-assessments when you join a company to determine that the work area is ergonomically fit, comfortable and appropriate for you. You may be able to request for an assessment if you have not had one or are having issues with your work environment
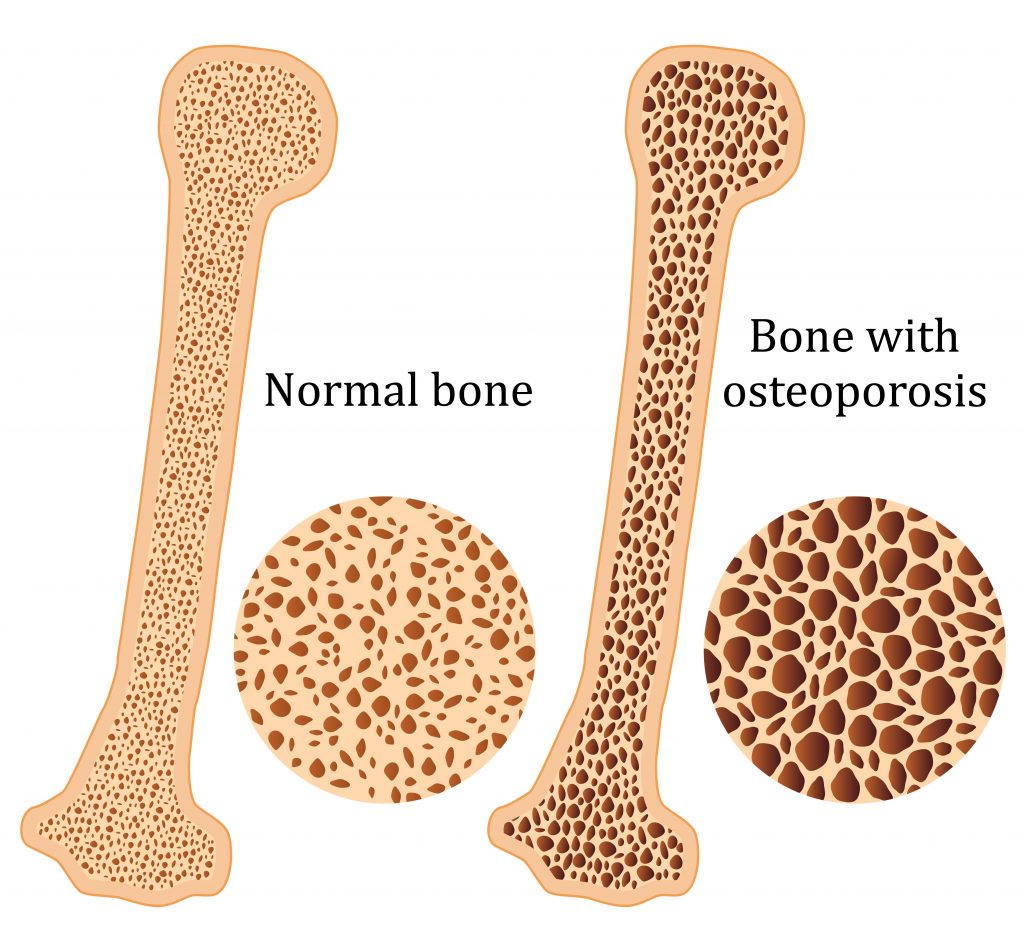
Osteoporosis is a condition which results in weak and brittle bones- to such degree that a fall or even mild stresses like coughing or bending over may result in a fracture. Bones are living tissues which are continually being broken down and replaced. However, your bones become osteoporotic when the formation of new bone does not keep up with the loss of old bone. This condition typically develops over time without any pain or other major symptoms, and is generally not diagnosed until you have sustained a fracture. The hip, pelvis, upper arm, spine and wrists are the most common structures affected by osteoporosis- related fractures.
How do you know if you have Osteoporosis?
Because there are no obvious early warning signs and symptoms, it is difficult to pre-diagnose osteoporosis. You may be unaware that you have this condition perhaps till you have one of the following:
Sustained a fracture from an incident more easily than you should have- like a simple fall or a bump
A decrease in the height of your spinal vertebrae over time
Change in posture – stooping or bending forwards
Back pain, due to a fractured or collapsed vertebra
Please see your doctor if you experience the following:
If you are over the age of 50 and have sustained a fracture
Sustained a spine, wrist, or hip for the first time
Sustained a fracture more easily than you should have (a simple fall or after a slight bump)
Risk factors
Key factors which may increase your risk of developing osteoporosis include:
Females- particularly post-menopausal Caucasian and Asian women
Over the age of 50
Excessive consumption of caffeine or alcohol
Smoking
Having a smaller or petite body frame
Poor physical activity levels and leading a very sedentary lifestyle
Family history of osteoporosis
Having low levels of vitamin D and poor dietary calcium intake
Decreasing levels of testosterone with ageing in men
Estrogen deficiency in women (irregular periods, early (before turning 40) or post-menopausal, surgical removal of the ovaries)
Use of long-term medication such as thyroid and epilepsy medications, corticosteroids
Having medical conditions such as gastrointestinal diseases; endocrine diseases; rheumatoid arthritis; cancer; and blood disorders
How will you be diagnosed?
Your doctor will review your signs and symptoms, family and medical history. You may be referred on for a specialized X-ray or CT scan to evaluate the bone density to help diagnose osteoporosis. Your bone density will be classified by comparing it to the typical bone density for a person of equivalent gender, size, and age.
How is Osteoporosis treated?
The treatment pathway chosen for the management of this condition is dependent on results of your bone density scan, gender, age, medical history and severity of the condition. Potential treatments for osteoporosis may include exercise, making positive lifestyle changes, vitamin and mineral supplements, and medications. Please consult your doctor for appropriate advice and treatment options.
How can Physiotherapy help?
Your physiotherapist will help you strengthen your bones and your muscles through a personalized and graduated rehabilitation program. Components of this rehabilitation program may include weightbearing aerobic exercises, resistance training using free weights/resistance bands/bodyweight resistance, and exercises to enhance posture, balance and body strength. Your physiotherapist will work with you to find activities that suit your needs and as per your physical activity level.
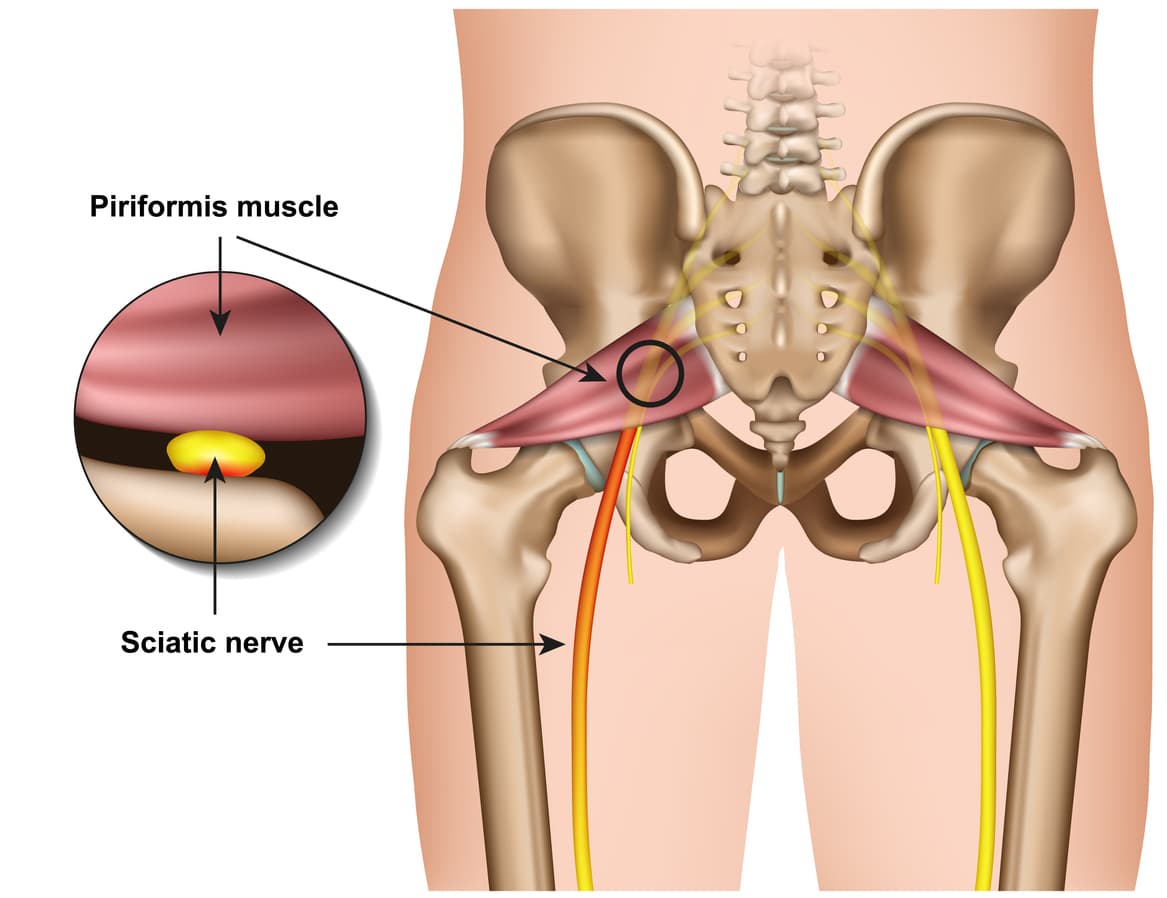
Piriformis syndrome refers to the dysfunction of the piriformis muscle which irritates the sciatic nerve. It is characterized by deep buttock region pain that radiates down leg and foot often accompanied by pins and needles and numbness traveling along the path of the sciatic nerve.
The simplistic reason for this widely distributed pain comes down to the piriformis muscle itself – Their close proximity means that direct trauma to the buttock region or the supporting structures can result in inflammation and muscle dysfunction which can compress and irritate the sciatic resulting in referred symptoms.
Piriformis syndrome symptoms may include:
Localised deep buttock region pain
Pain with continuous sitting or standing for 15 mins or over
Pins and needles along the leg down to the outer foot
Numbness in outer leg or foot (often resolves on movements)
Deep squatting or bending
Pain on direct palpation
Anatomy
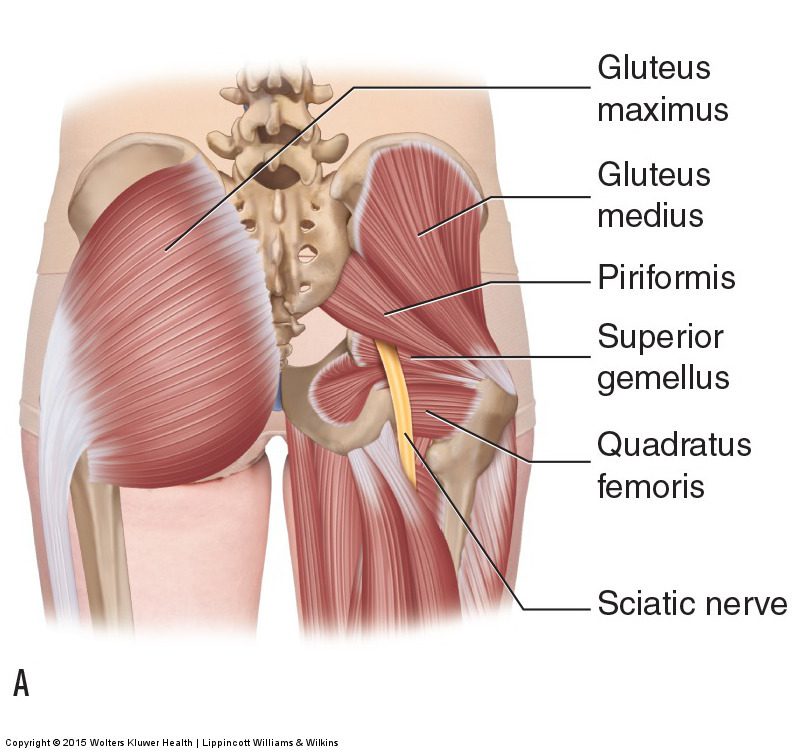
The piriformis muscle originates from the outer surface of a large fused bone of our pelvis called the sacrum. It travels adjacently and inserts into the top of the hip joint. The piriformis muscle is a very active muscle involved in stabilizing the hip and pelvis during majority of our activities (walking, running, standing, sitting or standing, turning in bed). When the piriformis muscle contracts it helps the hip rotate outwards (external rotation) and lift thigh out and up (abduct).
The sciatic nerve originates from where the very base of the spine and the sacrum join known as the lumbosacral region (lower back and saddle region). In this region five separate branches of nerves travel outside of the bony openings of the spine called the nerve roots and connect into a single large nerve – the sciatic nerve. It then travels through the pelvis deep into the buttock region close proximity the piriformis and gluteal muscles. In some individuals the piriformis muscles can travel through the piriformis muscle subjecting them to piriformis syndrome.
Diagnosis
There are no specific tests to diagnose piriformis syndrome. Diagnosis of piriformis syndrome is made by the report of symptoms and by physical exam using a variety of movements to elicit pain to the piriformis muscle. In some cases, a contracted or tender piriformis muscle can be found on physical exam.
In cases where there is underlying pathology (such as disc injury, arthritis, sacroiliac dysfunction or hip injury) resulting in true sciatica – piriformis syndrome may develop to become an additional muscular dysfunction that is required to be addressed. Because symptoms can be similar in other conditions, radiologic tests such as MRIs may be required to rule out other causes of sciatic nerve compression, such as a herniated disc.
Consultation with a physiotherapist in this case is highly recommended as they will perform a comprehensive clinical examination to identify the root cause of your symptoms.
Exercises for piriformis syndrome
Corrective exercises with a combination of strength and flexibility regimen is an essential way to treat true piriformis syndrome (without involvement of other underlying pathologies).
The exercises outlined below follow a phase-by-phase progressive regimen to strength key muscles of the hip, buttock and legs.
As you work through these exercises expect to feel some pain during and after your exercise. Pain you may feel during the exercise is an expected sign of muscle activity. Pain you may feel after the exercises is an expected sign of muscle healing and recovery. However, if you are unable to participate in the exercises due to symptom deterioration – it is highly recommended you consult your physiotherapist to rule out other potential causes.
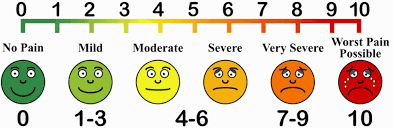
Otherwise, to help you gauge the correct amount of pain you should expect during exercise – use this scale. The ideal range should be 2 to 5. If your baseline pain is over 6 or 7 – it is recommended that you consult your doctor for pain relief appropriate to manage your pain, followed by a consult with a physiotherapist. Your physiotherapist will be able to modify the following exercises or prescribe alternative exercises best suited based on your current level of function and symptoms.
Symptom noting – is a great way to keep track of your progress and symptom behaviour.
Take a diary
Note down pain before you begin the exercise.
Note down the pain rating after each exercise.
Note down pain at the end of the day
Repeat the pain recording process for the next 4-5 days
Examine the trend in your symptoms.
Interference with everyday tasks – Your participation or level of exertion with everyday activities may interfere with your symptoms impacting your exercise tolerance. It is therefore important to note any of these interferences’ contributory to your pain.
Phase 1 – is a beginner stage.
This phase is intended for gently priming muscle activation. It will demand your concentration on technique and compliance to change the possible compensation your body has been used to as a result of pain. This phase can last between 1-2 weeks.
Instructions:
3 sets of 10 repetitions. Hold each repetition for 8-10 seconds. Rest 10-15 seconds between sets, 30 seconds between exercises. Do this exercise 1-2 times per day.
Bridges
Lie on your back.
Bend both knees and place your feet flat on the bed.
Lift your buttocks from the bed.
Place your buttocks back on the bed.
Repeat this exercise and remember to continue to breathe properly.
Clam shells
Lie on your side with your feet, ankles and knees together.
Bend the legs a little and tighten your core stability muscles.
Keeping the feet together, lift the top knee up.
Make sure you don’t roll your body back with the movement.
Control the movement as you bring the knee back down to the starting position.
Phase 2 – intermediate stage
The intermediate phase is similar to the beginner stage with the difference of using changing elements of progression to challenge the muscles capacity further. In this stage you may choose to progress the exercises by choosing to change ONE factor:
Increase repetitions
Increase hold time
Increase sets
Add appropriate resistance
Instructions:
3 sets of 10-15 repetitions. Hold each repetition for 10-15 seconds.
Rest 10-15 seconds between sets, 30 seconds between exercises.
Do this exercise 1-2 times per day.
Bridges with resistance
Tie a resistance band around both thighs, just above your knees.
Lie on your back with your knees bent and legs hips width apart.
There should be tension in the band.
Raise your hips up into a bridge, keeping the knees hips width apart.
Control the movement back down to the start position, maintaining constant tension on the band.
Clams with resistance
Lie on your side and place a band above your knees, approximately an inch or two above the knee joint.
Bend your legs a little, keeping the feet in line with your back.
Use your core stability muscles to keep the body stable.
Keeping your feet together, lift the top knee up against the resistance of the band.
Ensure you stay on your side and do not roll your hips and your body back with the movement.
Lower the knee back down, controlling the resistance.
Phase 3 – advance stage
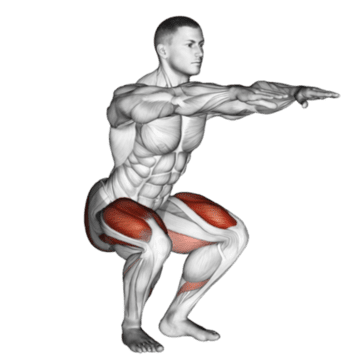
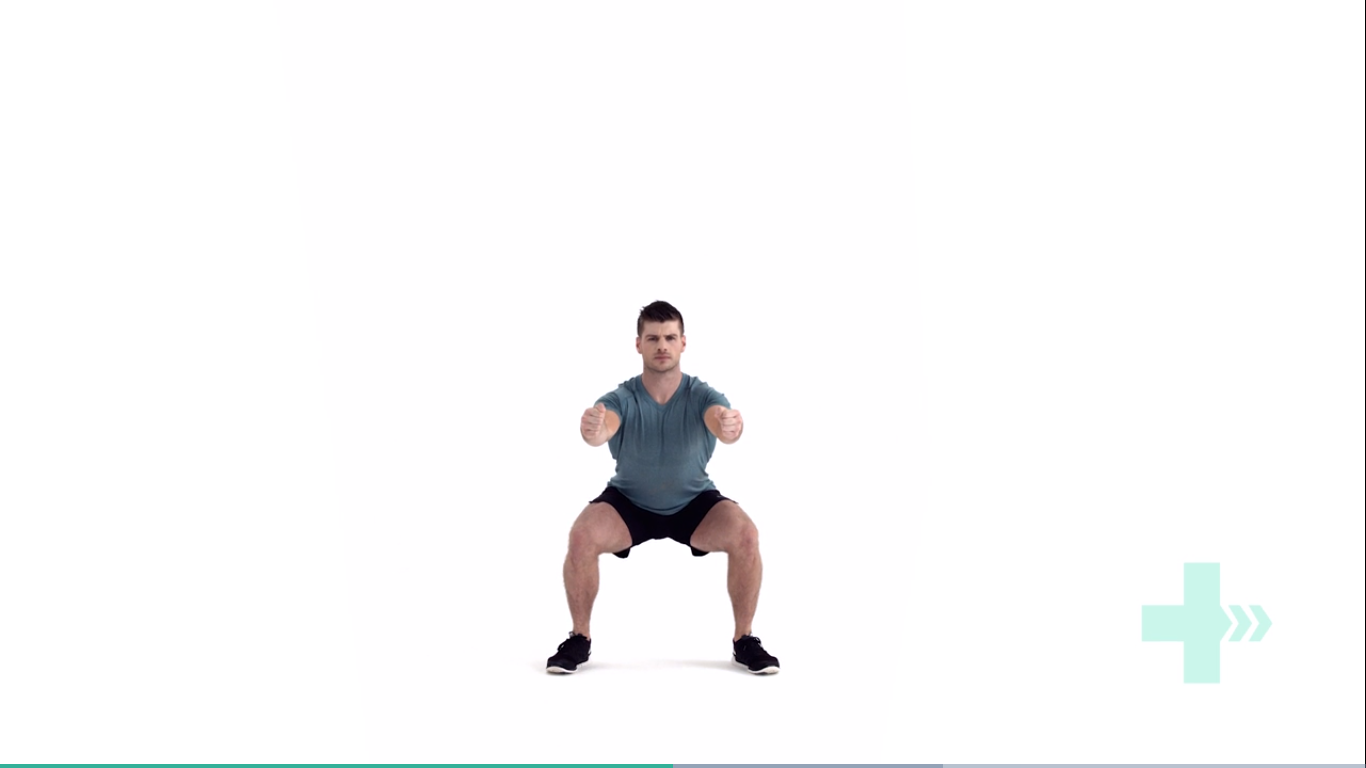
Body weight squats
Start position is standing straight with the arms out in front and bent at the elbows, the fists should be clenched and the palms facing inwards.
Move downwards into a squat position so that the knees are aligned over the toes and the heels are in contact with the floor, make sure the back is straight.
Keep the head and chest upright and the gaze horizontal.
Hold for 2 seconds and return to the start position.
Lunges
Stand straight with your arms to the side or on your hips.
Take a large step forwards on your affected leg, then drop your hips directly down between both feet, bending your hips and knees to a 90 degrees.
Push back up to the starting position, and repeat.
Make sure you take a large enough step that your front knee does not travel over your foot, and ensure your knee travels directly forwards.
Keep your body up straight throughout the movement.
Crab walks
Place a band around your ankles and gather some tension.
Side-step keeping constant tension on the band.
Make sure you do not bring your feet too close together and keep your toes and knees pointing forwards.
Phase 4 – return to activities
Stretching
Do you always need to stretch the muscle? The answer is NO. While stretching is an important tool to improve muscle elasticity. You may not always need to stretch a muscle if it is NOT tight. Thus, stretching is recommended to be limited to areas you feel are TIGHT when you perform a given movement. Check the affected side and unaffected side – don’t need to stretch a muscle that doesn’t need to be stretched.
Seated piriformis stretch
Start in a seated position.
Cross the symptomatic leg your ankle is resting on, to the opposite knee.
Apply gentle pressure to the knee as you lean forward, increasing the depth of the stretch.
Hold this position, you should feel a comfortable tension with no pain.
Pigeon stretch
Start on your hands and knees.
Cross the symptomatic leg underneath you, then lower your hips down to the ground.
Rest your body forwards on your arms.
You should feel a stretch across the buttock.
Although your knee has free movement going forwards and backwards, its’ sideward movements are restricted by the robust collateral ligaments on either sides of your knee. The medial collateral ligament (MCL) is situated on the inner part of your knee, but on the outside of your joint. The MCL connects the top of your shinbone (tibia) to the bottom of your femur (thighbone). It helps hold your bones together, provides stability and prevents your knee from bending sideways away from your body.
Injuries to the MCL are from the result of a direct blow to the outer part of your knee- and is most commonly seen in contact sports such as football and soccer. These injures may either over-stretch or cause a tear in the ligament. Whilst surgery may be needed in some severe cases, it is not always the go-to form of management.
Read on to know how physiotherapy can help manage your MCL related-knee pain.
Mechanism of Injury
Injury to the MCL typically occurs when a force drives the lower leg in a sideward direction away from your upper leg and body. Awkwardly landing from a height, twisting of your knee with your foot fixated to the ground, or from a direct blow to the outer part of your knee- most commonly seen in contact sports, are frequent causes of injury to the MCL.
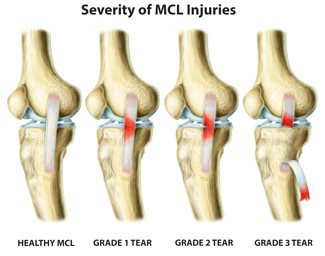
Grading of MCL Injuries
MCL injuries are often graded using the system below:
Grade 1: Regarded as a minor injury- means that the MCL has been overstretched but not torn
Grade 2: Regarded as a moderate injury- means that there is a partial tear in MCL, and presents with some degree of instability in the knee
Grade 3: Regarded as a severe injury- means that the MCL has completely ruptured/torn, and presents with noticeable joint instability
Often 3 MCL injuries are associated with concurrent medial meniscus and ACL ligament damage, which may need surgical intervention. But, the good news is that most MCL injuries may be treated well with conservative physiotherapy management. It usually takes between 2-8 weeks for Grade 1 and 2 MCL injuries to heal, and a graduated rehabilitation programme is highly commended for prevention of future injury.
Signs and Symptoms
Because injury to the MCL may present with similar symptoms as with other knee injuries such as ACL damage, it is vital to have a medical professional such as your physiotherapist evaluate your injury.
Common symptoms of an MCL injury may include:
Tenderness and pain along in the inner part of your knee
Swelling in the knee
Experience catching and locking sensations in the knee joint
A ‘pop’ sound at the time of injury
Actual or feeling of giving way of the knee (often indicate grade 2 or 3 injury)
Diagnosis
Your physiotherapist will discuss your injury and its presenting symptoms, past medical history (including a history of any prior knee injuries) and will also undertake a thorough physical examination. During the physical examination, your physiotherapist will assess the structures of your injured knee and compare them to the non-injured side. The range of motion, strength and stability of your knee will be assessed. You may be referred on for imaging such as X-rays and Ultrasounds to help aid the diagnosis. For more severe MCL injuries, and if your symptoms do not resolve with conservative physiotherapy management, you may be referred onto a specialist who may consider referring you for an MRI to get a deeper look at your knee.
Management
The management options for MCL injuries will be dependent on the severity of the injury. In the initial stages of injury, management is focused on controlling swelling and pain, whilst allowing your body to initiate healing processes via inflammation. This is typically achieved through the P.O.L.I.C.E. principles (Protect, Optimal Loading, Ice, Compression and Elevation).
Over the counter medication such as ibuprofen and paracetamol may be taken to reduce pain. Other stronger painkillers and NSAIDs may be prescribed by your doctor to help reduce swelling and inflammation as well.
After assessing your knee, your physiotherapist will frame a rehabilitation programme with exercises tailored to your needs. The purpose of physiotherapy is to help restore your knee’s range of motion, stability and strength, which in turn will then allow you to safely return to your usual day-to-day and sporting activities as soon as possible.
Management of most MCL injuries usually only involves knee bracing and physiotherapy treatment. However, in some cases, surgery may be recommended. Particularly if there is damage to more than one ligament or structure in your knee or if you continue to experience instability in spite of physiotherapy.